Department of Gastroenterology and Hepatology, University of Amsterdam, Amsterdam, The Netherlands.
BMC Gastroenterol. 2013 Nov 25;13:161. doi: 10.1186/1471-230X-13-161.
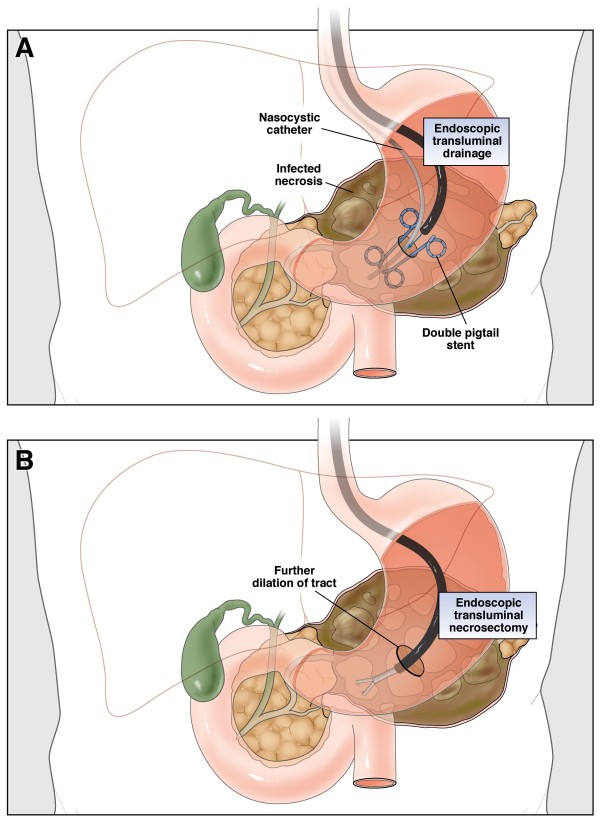
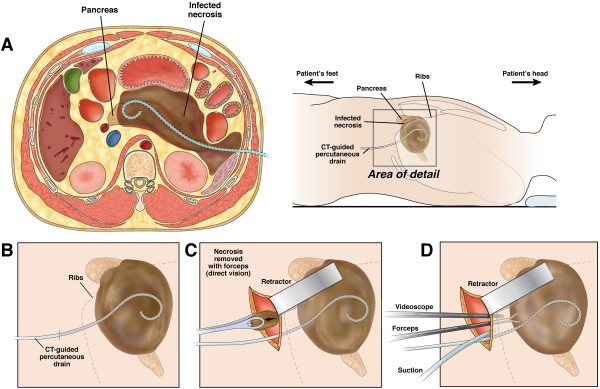
Infected necrotising pancreatitis is a potentially lethal disease that nearly always requires intervention. Traditionally, primary open necrosectomy has been the treatment of choice. In recent years, the surgical step-up approach, consisting of percutaneous catheter drainage followed, if necessary, by (minimally invasive) surgical necrosectomy has become the standard of care. A promising minimally invasive alternative is the endoscopic transluminal step-up approach. This approach consists of endoscopic transluminal drainage followed, if necessary, by endoscopic transluminal necrosectomy. We hypothesise that the less invasive endoscopic step-up approach is superior to the surgical step-up approach in terms of clinical and economic outcomes.
METHODS/DESIGN: The TENSION trial is a randomised controlled, parallel-group superiority multicenter trial. Patients with (suspected) infected necrotising pancreatitis with an indication for intervention and in whom both treatment modalities are deemed possible, will be randomised to either an endoscopic transluminal or a surgical step-up approach. During a 4 year study period, 98 patients will be enrolled from 24 hospitals of the Dutch Pancreatitis Study Group. The primary endpoint is a composite of death and major complications within 6 months following randomisation. Secondary endpoints include complications such as pancreaticocutaneous fistula, exocrine or endocrine pancreatic insufficiency, need for additional radiological, endoscopic or surgical intervention, the need for necrosectomy after drainage, the number of (re-)interventions, quality of life, and total direct and indirect costs.
The TENSION trial will answer the question whether an endoscopic step-up approach reduces the combined primary endpoint of death and major complications, as well as hospital stay and related costs compared with a surgical step-up approach in patients with infected necrotising pancreatitis.
感染性坏死性胰腺炎是一种潜在致命的疾病,几乎总是需要干预。传统上,开放性坏死性胰腺切除术一直是首选治疗方法。近年来,外科逐步升级治疗方法,包括经皮导管引流,如果需要,随后进行(微创)手术坏死性胰腺切除术,已成为治疗标准。一种有前途的微创替代方法是内镜经腔逐步升级治疗方法。这种方法包括内镜经腔引流,如果需要,随后进行内镜经腔坏死性胰腺切除术。我们假设,在临床和经济结果方面,微创内镜逐步升级治疗方法优于外科逐步升级治疗方法。
方法/设计:TENSION 试验是一项随机对照、平行组优效性多中心试验。患有(疑似)感染性坏死性胰腺炎且需要干预,并且两种治疗方法都被认为可行的患者,将被随机分配到内镜经腔或外科逐步升级治疗方法。在 4 年的研究期间,将从荷兰胰腺炎研究组的 24 家医院招募 98 名患者。主要终点是随机分组后 6 个月内死亡和主要并发症的复合结果。次要终点包括胰腺皮瘘、外分泌或内分泌胰腺功能不全、需要额外的放射学、内镜或手术干预、引流后需要坏死性胰腺切除术、(再)干预次数、生活质量以及直接和间接总费用。
TENSION 试验将回答以下问题:在感染性坏死性胰腺炎患者中,与外科逐步升级治疗方法相比,内镜逐步升级治疗方法是否能降低死亡和主要并发症的联合主要终点,以及住院时间和相关费用。