Suraj Eye Institute, Nagpur, India ; Department of Ophthalmology, Medical Faculty Mannheim of the Ruprecht-Karls-University of Heidelberg, Mannheim, Germany.
PLoS One. 2013 Dec 6;8(12):e82284. doi: 10.1371/journal.pone.0082284. eCollection 2013.
To assess associations of the trans-lamina cribrosa pressure difference (TLCPD) with glaucomatous optic neuropathy.
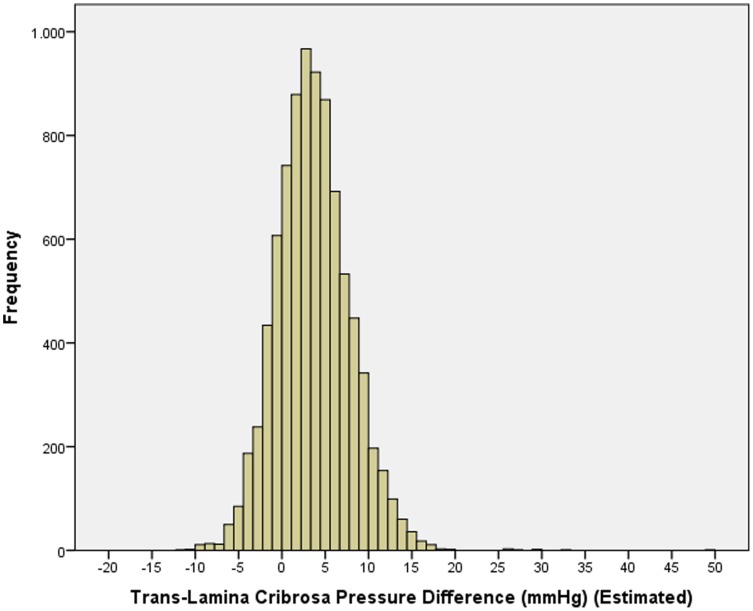
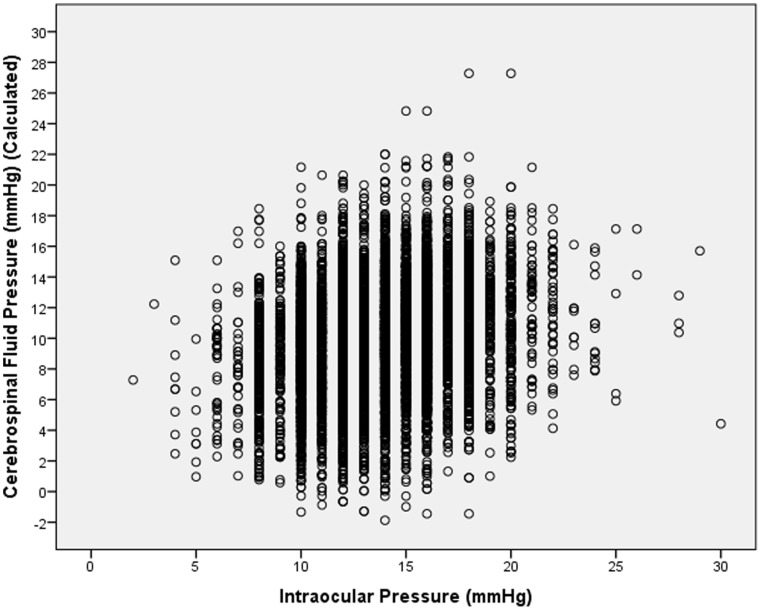
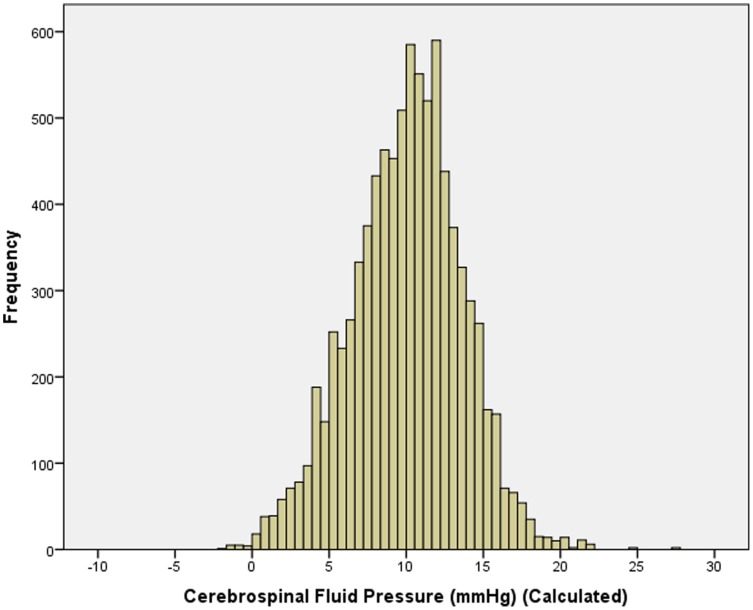
The population-based Central India Eye and Medical Study included 4711 subjects. Based on a previous study with lumbar cerebrospinal fluid pressure (CSFP) measurements, CSFP was calculated as CSFP[mmHg] = 0.44 Body Mass Index[kg/m2]+0.16 Diastolic Blood Pressure[mmHg]-0.18×Age[Years] -1.91. TLCPD was IOP-CSFP.
Mean TLCPD was 3.64±4.25 mm Hg in the non-glaucomatous population and 9.65±8.17 mmHg in the glaucomatous group. In multivariate analysis, TLCPD was associated with older age (P<0.001; standardized coefficient beta:0.53; regression coefficient B:0.18; 95% confidence interval (CI):0.17, 0.18), lower body mass index (P<0.001; beta: -0.28; B: -0.36; 95%CI: -0.38, -0.31), lower diastolic blood pressure (P<0.001; beta: -0.31; B: -0.12; 95%CI: -0.13, -0.11), higher pulse (P<0.001; beta:0.05; B:0.02; 95%CI:0.01,0.2), lower body height (P = 0.02; beta: -0.02; B: -0.01; 95%CI: -0.02,0.00), higher educational level (P<0.001; beta:0.04; B:0.15; 95%CI:0.09,0.22), higher cholesterol blood concentrations (P<0.001; beta:0.04; B:0.01; 95%CI:0.01,0.01), longer axial length (P = 0.006; beta:0.03; B:0.14; 95%CI:0.04,0.24), thicker central cornea (P<0.001; beta:0.15; B:0.02; 95%CI:0.02,0.02), higher corneal refractive power (P<0.001; beta:0.07; B:0.18; 95%CI:0.13,0.23) and presence of glaucomatous optic neuropathy (P<0.001; beta:0.11; B:3.43; 95%CI:2.96,3.99). Differences between glaucomatous subjects and non-glaucomatous subjects in CSFP were more pronounced for open-angle glaucoma (OAG) than for angle-closure glaucoma (ACG) (3.0 mmHg versus 1.8 mmHg), while differences between glaucomatous subjects and non-glaucomatous subjects in IOP were higher for ACG than for OAG (8.5 mmHg versus 3.0 mmHg). Presence of OAG was significantly associated with TLCPD (P<0.001; OR:1.24; 95%CI:1.19,1.29) but not with IOP (P = 0.08; OR:0.96; 95%CI:0.91,1.00). Prevalence of ACG was significantly associated with IOP (P = 0.04; OR:1.19; 95%CI:1.01,1.40) but not with TLCPD (P = 0.92).
In OAG, but not in ACG, calculated TLCPD versus IOP showed a better association with glaucoma presence and amount of glaucomatous optic neuropathy. It supports the notion of a potential role of low CSFP in the pathogenesis of open-angle glaucoma.
评估跨脊筛板压力差(TLCPD)与青光眼视神经病变的相关性。
本研究基于中央印度眼与医学研究的人群基础,共纳入 4711 名受试者。根据之前的腰椎脑脊液压力(CSFP)测量研究,CSFP 计算为 CSFP[mmHg] = 0.44 体重指数[kg/m2] + 0.16 舒张压[mmHg] - 0.18×年龄[岁] - 1.91。TLCPD 为 IOP-CSFP。
在非青光眼人群中,平均 TLCPD 为 3.64±4.25mmHg,而在青光眼组中为 9.65±8.17mmHg。在多变量分析中,TLCPD 与年龄较大(P<0.001;标准化系数β:0.53;回归系数 B:0.18;95%置信区间(CI):0.17,0.18)、较低的体重指数(P<0.001;β:-0.28;B:-0.36;95%CI:-0.38,-0.31)、较低的舒张压(P<0.001;β:-0.31;B:-0.12;95%CI:-0.13,-0.11)、较高的脉搏(P<0.001;β:0.05;B:0.02;95%CI:0.01,0.2)、较低的身高(P=0.02;β:-0.02;B:-0.01;95%CI:-0.02,0.00)、较高的教育水平(P<0.001;β:0.04;B:0.15;95%CI:0.09,0.22)、较高的胆固醇血浓度(P<0.001;β:0.04;B:0.01;95%CI:0.01,0.01)、较长的眼轴长度(P=0.006;β:0.03;B:0.14;95%CI:0.04,0.24)、较厚的中央角膜(P<0.001;β:0.15;B:0.02;95%CI:0.02,0.02)、较高的角膜屈光力(P<0.001;β:0.07;B:0.18;95%CI:0.13,0.23)和青光眼视神经病变的存在(P<0.001;β:0.11;B:3.43;95%CI:2.96,3.99)有关。与非青光眼受试者相比,开角型青光眼(OAG)患者的 CSFP 差异比闭角型青光眼(ACG)更为明显(3.0mmHg 比 1.8mmHg),而与非青光眼受试者相比,ACG 患者的 IOP 差异比 OAG 更为明显(8.5mmHg 比 3.0mmHg)。OAG 的存在与 TLCPD 显著相关(P<0.001;OR:1.24;95%CI:1.19,1.29),但与 IOP 无关(P=0.08;OR:0.96;95%CI:0.91,1.00)。ACG 的患病率与 IOP 显著相关(P=0.04;OR:1.19;95%CI:1.01,1.40),但与 TLCPD 无关(P=0.92)。
在 OAG 中,而不是在 ACG 中,计算的 TLCPD 与 IOP 与青光眼的存在和青光眼视神经病变的严重程度有更好的相关性。这支持了低 CSFP 在开角型青光眼发病机制中的潜在作用的观点。