Rankin J S, Daneshmand M A, Milano C A, Gaca J G, Glower D D, Smith P K
Centennial Medical Center and Vanderbilt University, Nashville, TN.
Division of Cardiothoracic Surgery, Duke University Medical Center, Durham, NC.
Heart Lung Vessel. 2013;5(4):246-51.
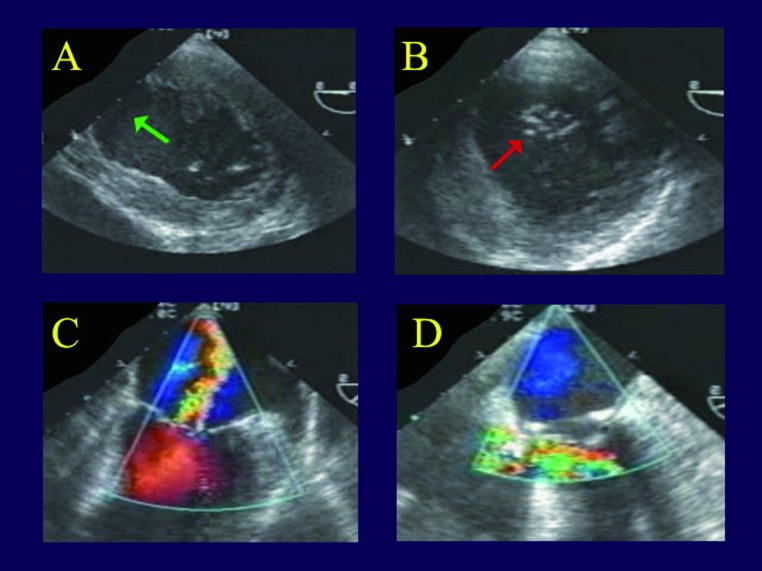
Ischemic mitral regurgitation can be defined as moderate to severe mitral leak precipitated by acute myocardial infarction. Valve repair is now the procedure of choice, but some cases can pose difficult anatomy. This review will illustrate current techniques for repairing complex ischemic mitral regurgitation.
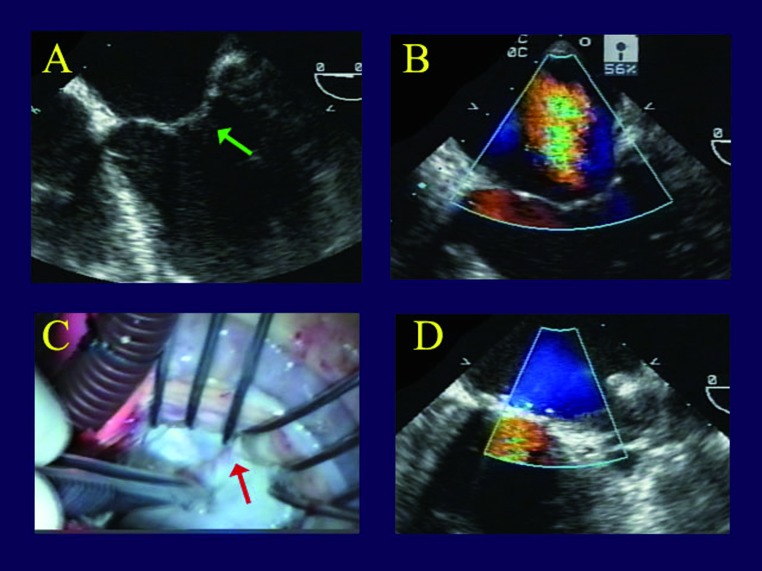
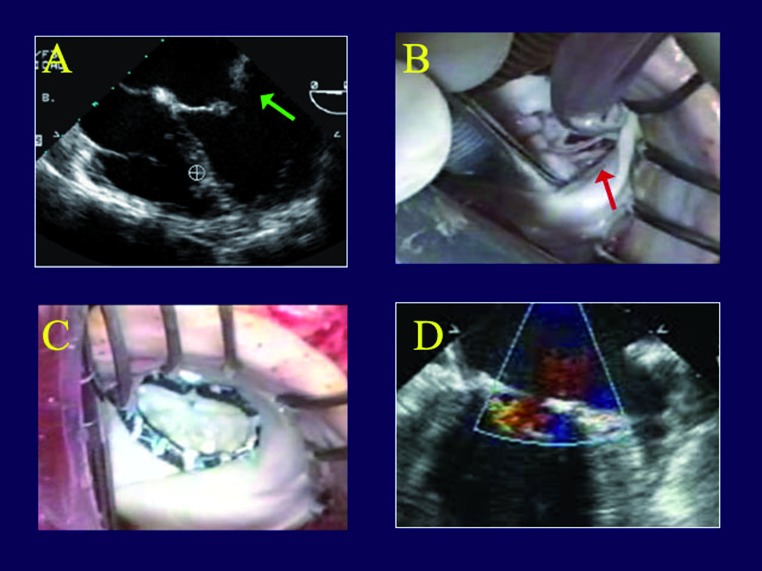
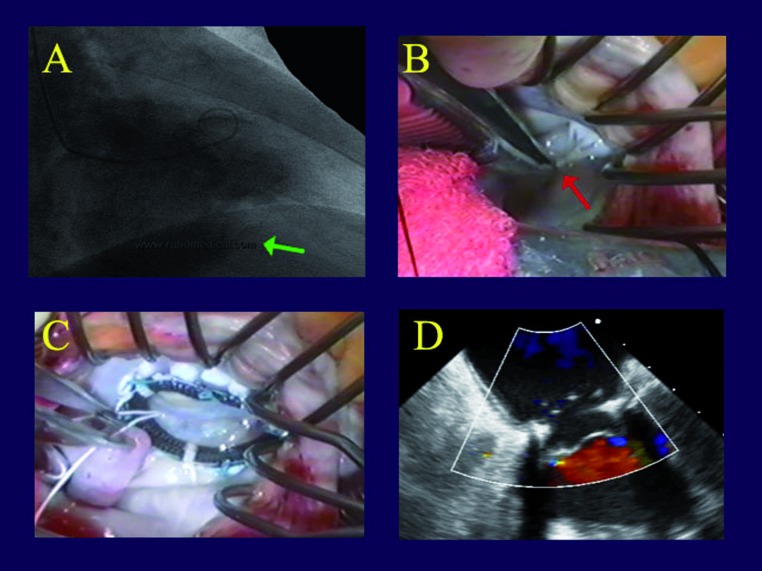
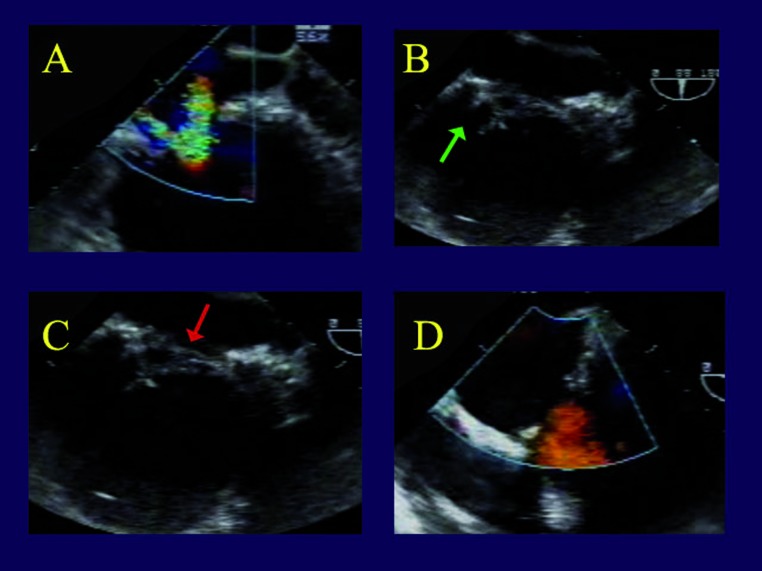
Most patients with ischemic mitral regurgitation have predominant annular dilatation at the posterior commissure and require only ring annuloplasty. Full rigid rings are used preferentially. With leaflet tethering, adjunctive autologous pericardial patches are effective in restoring leaflet coaptation. If papillary muscle elongation or rupture occurs, Gore-Tex artificial chordal replacement performs well. With ischemic mitral regurgitation accompanying posterior ventricular aneurysms, standard trans-atrial mitral repair provides the best results, with associated aneurysms being repaired concurrently.
Surgical approaches and technical outcomes of mitral repair in ischemic mitral regurgitation are illustrated in 5 patients using operative images and echocardiograms. Each method is illustrated, including ring annuloplasty, pericardial leaflet augmentation, artificial chordal replacement, and ventricular aneurysm repair. Using these techniques, virtually all ischemic mitral regurgitation can be repaired, with consequential patient benefits, even in the most complex anatomy.
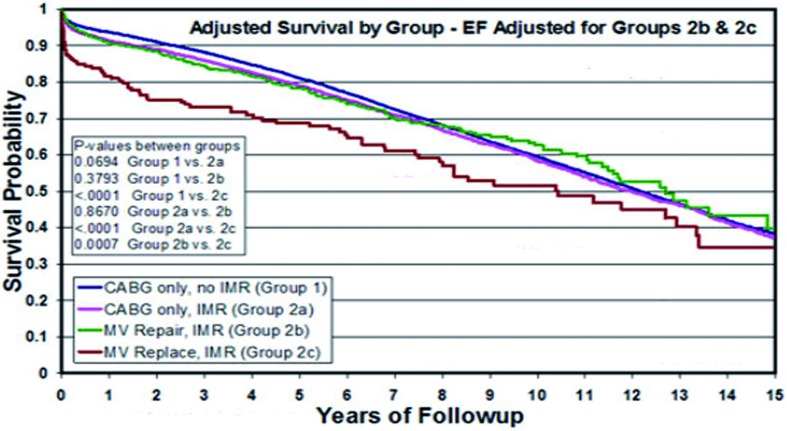
Ischemic mitral regurgitation has been shown to have better outcomes when managed with valve repair. Using combinations of annular, leaflet, and chordal procedures, even complex ischemic mitral regurgitation can undergo autologous reconstruction with excellent long-term results.
缺血性二尖瓣反流可定义为由急性心肌梗死引发的中度至重度二尖瓣漏。瓣膜修复目前是首选手术方式,但有些病例的解剖结构较为复杂。本综述将阐述修复复杂性缺血性二尖瓣反流的当前技术。
大多数缺血性二尖瓣反流患者在后叶交界处主要存在瓣环扩张,仅需进行瓣环成形术。优先使用全硬质瓣环。对于瓣叶受限,自体心包补片辅助可有效恢复瓣叶对合。若发生乳头肌延长或断裂,使用戈尔特斯(Gore-Tex)人工腱索置换效果良好。对于伴有后室壁瘤的缺血性二尖瓣反流,标准经心房二尖瓣修复效果最佳,同时可一并修复相关室壁瘤。
通过手术图像和超声心动图展示了5例缺血性二尖瓣反流患者二尖瓣修复的手术入路和技术效果。阐述了每种方法,包括瓣环成形术、心包瓣叶扩大术、人工腱索置换和室壁瘤修复。使用这些技术,几乎所有缺血性二尖瓣反流均可修复,从而使患者受益,即便在解剖结构最为复杂的情况下亦是如此。
已证实缺血性二尖瓣反流采用瓣膜修复治疗效果更佳。通过联合应用瓣环、瓣叶和腱索手术,即使是复杂的缺血性二尖瓣反流也可进行自体重建并获得优异的长期效果。