Magnusson Erik, Cao Qing, Linden Michael A, Frolich Jerry, Anand Vidhu, Burns Linda J, Bachanova Veronika
Division of Hematology-Oncology and Transplantation, University of Minnesota, Minneapolis, MN.
Division of Hematopathology, Department of Laboratory Medicine and Pathology, University of Minnesota, Minneapolis, MN.
Clin Lymphoma Myeloma Leuk. 2014 Apr;14(2):114-21. doi: 10.1016/j.clml.2013.10.007. Epub 2013 Nov 15.
The prognostic roles of 18F-fludeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) imaging and marrow involvement evaluation on outcomes following autologous and allogeneic hematopoietic cell transplantation (HCT) for mantle cell lymphoma (MCL) are uncertain and require more data.
We categorized 66 patients with MCL who received HCT (38 autologous and 28 allogeneic) on the basis of pre-HCT residual disease (RD) status as assessed by marrow MCL morphology and flow/molecular analysis and PET/CT imaging to RD positive (RD(+)) (either or both measures positive) and RD(-) (both negative). We analyzed the predictive value of these RD detection methods on transplant outcomes.
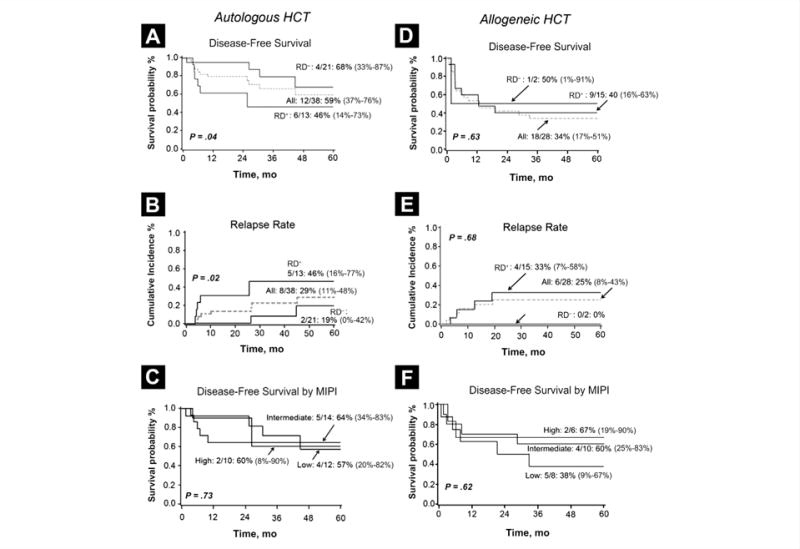
The 2-year relapse rate after autograft was significantly higher in pre-HCT RD(+) patients (46% [95% CI 16-77%]) than in patients who were RD(-) (19% [95% CI 0-42%]; P = .02), leading to worse 5-year disease-free survival (DFS) in RD(+) patients (46% [95% CI 14%-73%] vs. 68% [95% CI 33-87%], P = .04). In multivariate analysis, RD(+) status was associated with a reduction in DFS (hazard ratio, 5.6; P = .02). Most allogeneic HCT recipients had advanced disease and most were RD(+) (12 PET/CT(+); 5 marrow-positive). The 5-year DFS and relapse rates after allogeneic HCT were 34% and 25% for all patients and 40% and 33% for RD(+) recipients, suggesting that active disease at the time of allograft does not preclude long-term remissions in advanced MCL.
Both autologous and allogeneic HCT lead to promising long-term survival. RD detected prior to autograft was associated with increased relapse and worse 5 year DFS. Allograft recipients had favorable long-term outcomes even in presence of pre-HCT detectable disease.
18F-氟脱氧葡萄糖(FDG)正电子发射断层扫描/计算机断层扫描(PET/CT)成像以及骨髓受累评估在套细胞淋巴瘤(MCL)自体和异基因造血细胞移植(HCT)后的预后作用尚不确定,需要更多数据。
我们根据骨髓MCL形态学以及流式/分子分析和PET/CT成像评估的移植前残留疾病(RD)状态,将66例接受HCT的MCL患者(38例自体移植和28例异基因移植)分为RD阳性(RD(+))(任何一种或两种检测均为阳性)和RD阴性(RD(-))(两种检测均为阴性)。我们分析了这些RD检测方法对移植结局的预测价值。
自体移植后,移植前RD(+)患者的2年复发率(46% [95% CI 16 - 77%])显著高于RD(-)患者(19% [95% CI 0 - 42%];P = 0.02),导致RD(+)患者的5年无病生存率(DFS)更差(46% [95% CI 14% - 73%] 对 68% [95% CI 33 - 87%],P = 0.04)。多因素分析中,RD(+)状态与DFS降低相关(风险比,5.6;P = 0.02)。大多数异基因HCT受者疾病处于晚期,且大多数为RD(+)(12例PET/CT(+);5例骨髓阳性)。异基因HCT后所有患者的5年DFS和复发率分别为34%和25%,RD(+)受者分别为40%和33%,这表明同种异体移植时的活动性疾病并不排除晚期MCL患者的长期缓解。
自体和异基因HCT均能带来有希望的长期生存。自体移植前检测到的RD与复发增加及5年DFS较差相关。即使存在移植前可检测到的疾病,异基因移植受者仍有良好的长期结局。