Ellis Amanda, Wieseler Julie, Favret Jacob, Johnson Kirk W, Rice Kenner C, Maier Steven F, Falci Scott, Watkins Linda R
Department of Psychology and Neuroscience, University of Colorado Boulder, Boulder, Colorado.
Department of Psychology and Neuroscience, University of Colorado Boulder, Boulder, Colorado.
J Pain. 2014 Apr;15(4):407-21. doi: 10.1016/j.jpain.2013.12.007. Epub 2014 Jan 9.
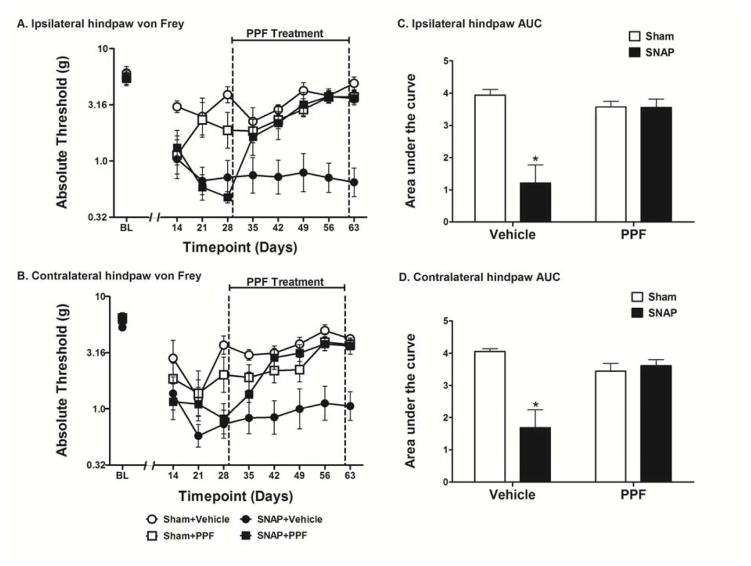
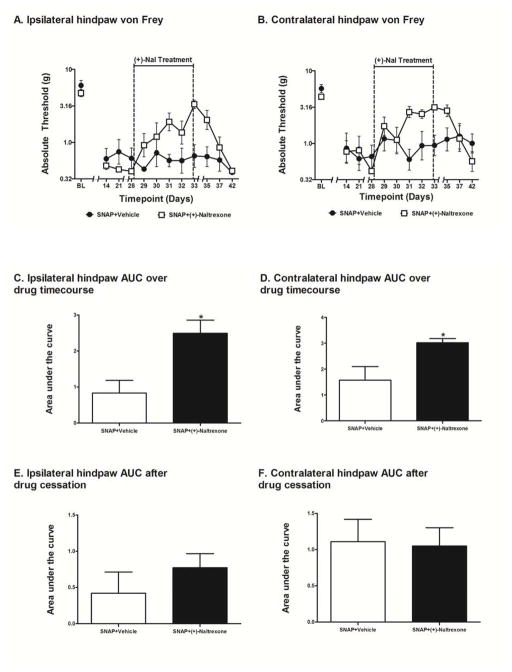
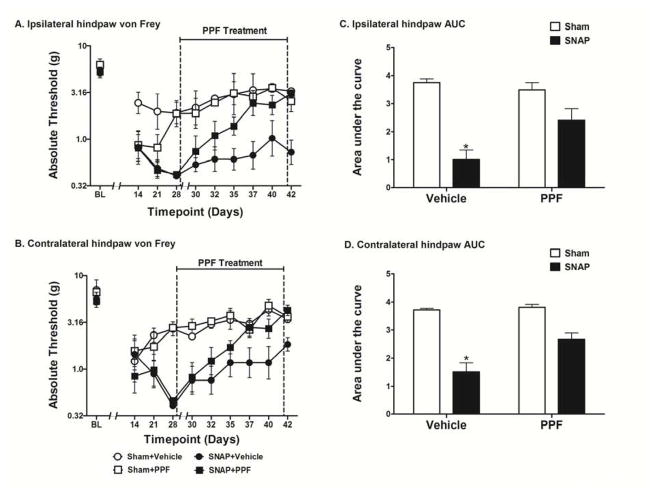
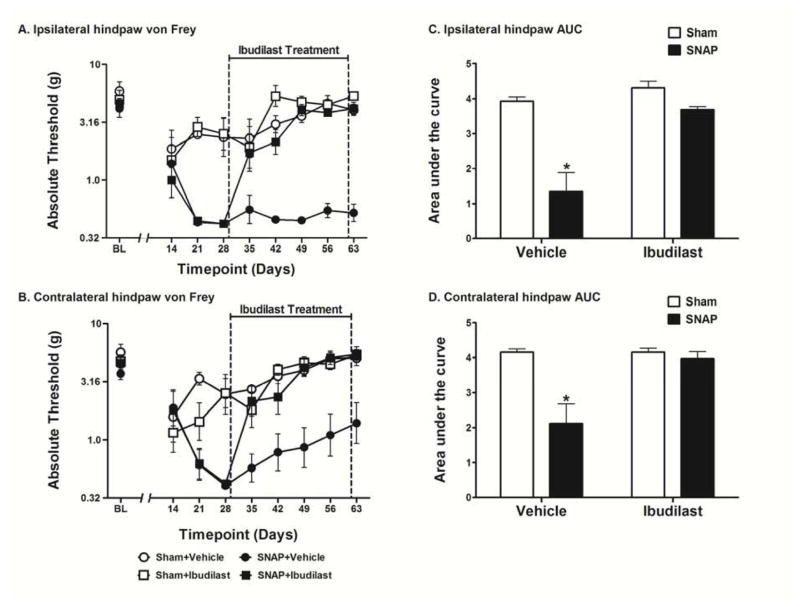
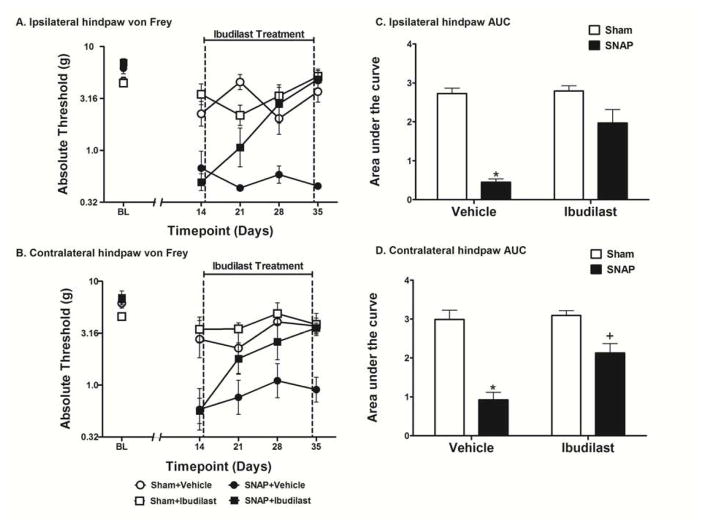
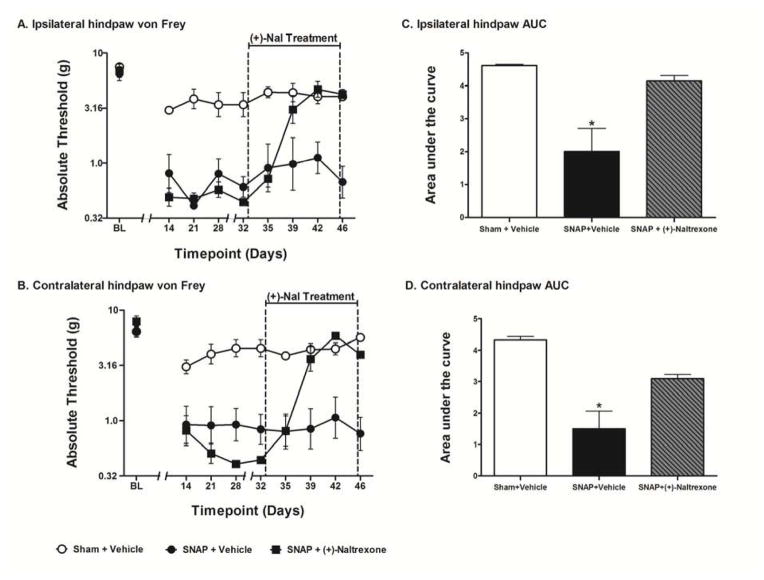
Central neuropathic pain (CNP) is a debilitating consequence of central nervous system damage for which current treatments are ineffective. To explore mechanisms underlying CNP, we developed a rat model involving T13/L1 dorsal root avulsion. The resultant dorsal horn damage creates bilateral below-level (L4-L6) mechanical allodynia. This allodynia, termed spinal neuropathic avulsion pain, occurs in the absence of confounding paralysis. To characterize this model, we undertook a series of studies aimed at defining whether spinal neuropathic avulsion pain could be reversed by any of 3 putative glial activation inhibitors, each with distinct mechanisms of action. Indeed, the phosphodiesterase inhibitor propentofylline, the macrophage migration inhibitory factor inhibitor ibudilast, and the toll-like receptor 4 antagonist (+)-naltrexone each reversed below-level allodynia bilaterally. Strikingly, none of these impacted spinal neuropathic avulsion pain upon first administration but required 1 to 2 weeks of daily administration before pain reversal was obtained. Given reversal of CNP by each of these glial modulatory agents, these results suggest that glia contribute to the maintenance of such pain and enduring release of macrophage migration inhibitory factor and endogenous agonists of toll-like receptor 4 is important for sustaining CNP. The markedly delayed efficacy of all 3 glial modulatory drugs may prove instructive for interpretation of apparent drug failures after shorter dosing regimens.
CNP that develops after trauma is often described by patients as severe and intolerable. Unfortunately, current treatments are not effective. This work suggests that using pharmacologic treatments that target glial cells could be an effective clinical treatment for CNP.
中枢神经性疼痛(CNP)是中枢神经系统损伤导致的一种使人衰弱的后果,目前的治疗方法对此无效。为了探究CNP的潜在机制,我们建立了一种涉及T13/L1背根撕脱的大鼠模型。由此产生的背角损伤导致双侧L4-L6水平以下出现机械性异常性疼痛。这种异常性疼痛,称为脊髓神经性撕脱痛,在没有混杂性麻痹的情况下发生。为了表征该模型,我们进行了一系列研究,旨在确定脊髓神经性撕脱痛是否可以被三种假定的神经胶质激活抑制剂中的任何一种逆转,每种抑制剂都有不同的作用机制。事实上,磷酸二酯酶抑制剂丙戊茶碱、巨噬细胞迁移抑制因子抑制剂异丁司特和Toll样受体4拮抗剂(+)-纳曲酮均可双侧逆转L4-L6水平以下的异常性疼痛。令人惊讶的是,这些药物在首次给药时均未影响脊髓神经性撕脱痛,但需要连续1至2周每日给药才能使疼痛得到逆转。鉴于这些神经胶质调节药物均可逆转CNP,这些结果表明神经胶质细胞有助于维持此类疼痛,巨噬细胞迁移抑制因子的持续释放以及Toll样受体4的内源性激动剂对于维持CNP很重要。所有三种神经胶质调节药物明显延迟的疗效可能对解释较短给药方案后明显的药物失败具有指导意义。
创伤后发生的CNP通常被患者描述为严重且难以忍受。不幸的是,目前的治疗方法无效。这项研究表明,使用针对神经胶质细胞的药物治疗可能是治疗CNP的有效临床方法。