Steingart Karen R, Schiller Ian, Horne David J, Pai Madhukar, Boehme Catharina C, Dendukuri Nandini
Cochrane Infectious Diseases Group, Liverpool School of Tropical Medicine, Pembroke Place, Liverpool, UK.
Cochrane Database Syst Rev. 2014 Jan 21;2014(1):CD009593. doi: 10.1002/14651858.CD009593.pub3.
Accurate, rapid detection of tuberculosis (TB) and TB drug resistance is critical for improving patient care and decreasing TB transmission. Xpert® MTB/RIF assay is an automated test that can detect both TB and rifampicin resistance, generally within two hours after starting the test, with minimal hands-on technical time. The World Health Organization (WHO) issued initial recommendations on Xpert® MTB/RIF in early 2011. A Cochrane Review on the diagnostic accuracy of Xpert® MTB/RIF for pulmonary TB and rifampicin resistance was published January 2013. We performed this updated Cochrane Review as part of a WHO process to develop updated guidelines on the use of the test.
To assess the diagnostic accuracy of Xpert® MTB/RIF for pulmonary TB (TB detection), where Xpert® MTB/RIF was used as both an initial test replacing microscopy and an add-on test following a negative smear microscopy result.To assess the diagnostic accuracy of Xpert® MTB/RIF for rifampicin resistance detection, where Xpert® MTB/RIF was used as the initial test replacing culture-based drug susceptibility testing (DST).The populations of interest were adults presumed to have pulmonary, rifampicin-resistant or multidrug-resistant TB (MDR-TB), with or without HIV infection. The settings of interest were intermediate- and peripheral-level laboratories. The latter may be associated with primary health care facilities.
We searched for publications in any language up to 7 February 2013 in the following databases: Cochrane Infectious Diseases Group Specialized Register; MEDLINE; EMBASE; ISI Web of Knowledge; MEDION; LILACS; BIOSIS; and SCOPUS. We also searched the metaRegister of Controlled Trials (mRCT) and the search portal of the WHO International Clinical Trials Registry Platform to identify ongoing trials.
We included randomized controlled trials, cross-sectional studies, and cohort studies using respiratory specimens that allowed for extraction of data evaluating Xpert® MTB/RIF against the reference standard. We excluded gastric fluid specimens. The reference standard for TB was culture and for rifampicin resistance was phenotypic culture-based DST.
For each study, two review authors independently extracted data using a standardized form. When possible, we extracted data for subgroups by smear and HIV status. We assessed the quality of studies using QUADAS-2 and carried out meta-analyses to estimate pooled sensitivity and specificity of Xpert® MTB/RIF separately for TB detection and rifampicin resistance detection. For TB detection, we performed the majority of analyses using a bivariate random-effects model and compared the sensitivity of Xpert® MTB/RIF and smear microscopy against culture as reference standard. For rifampicin resistance detection, we undertook univariate meta-analyses for sensitivity and specificity separately to include studies in which no rifampicin resistance was detected.
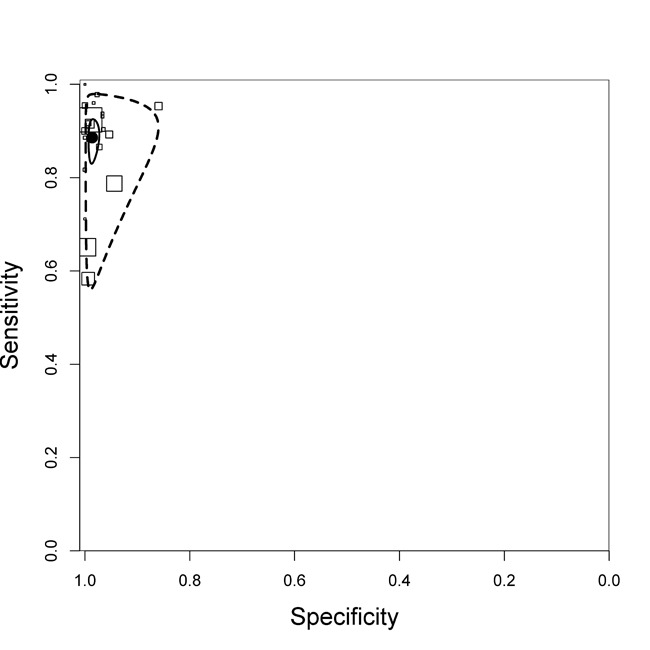
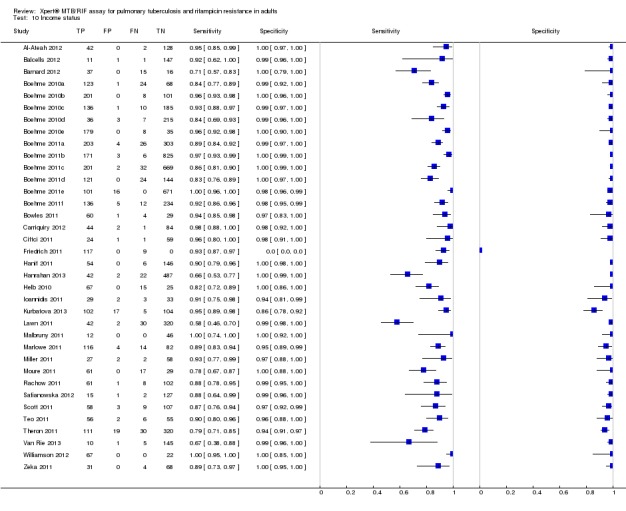
We included 27 unique studies (integrating nine new studies) involving 9557 participants. Sixteen studies (59%) were performed in low- or middle-income countries. For all QUADAS-2 domains, most studies were at low risk of bias and low concern regarding applicability.As an initial test replacing smear microscopy, Xpert® MTB/RIF pooled sensitivity was 89% [95% Credible Interval (CrI) 85% to 92%] and pooled specificity 99% (95% CrI 98% to 99%), (22 studies, 8998 participants: 2953 confirmed TB, 6045 non-TB).As an add-on test following a negative smear microscopy result, Xpert®MTB/RIF pooled sensitivity was 67% (95% CrI 60% to 74%) and pooled specificity 99% (95% CrI 98% to 99%; 21 studies, 6950 participants).For smear-positive, culture-positive TB, Xpert® MTB/RIF pooled sensitivity was 98% (95% CrI 97% to 99%; 21 studies, 1936 participants).For people with HIV infection, Xpert® MTB/RIF pooled sensitivity was 79% (95% CrI 70% to 86%; 7 studies, 1789 participants), and for people without HIV infection, it was 86% (95% CrI 76% to 92%; 7 studies, 1470 participants). Comparison with smear microscopy In comparison with smear microscopy, Xpert® MTB/RIF increased TB detection among culture-confirmed cases by 23% (95% CrI 15% to 32%; 21 studies, 8880 participants).For TB detection, if pooled sensitivity estimates for Xpert® MTB/RIF and smear microscopy are applied to a hypothetical cohort of 1000 patients where 10% of those with symptoms have TB, Xpert® MTB/RIF will diagnose 88 cases and miss 12 cases, whereas sputum microscopy will diagnose 65 cases and miss 35 cases. Rifampicin resistance For rifampicin resistance detection, Xpert® MTB/RIF pooled sensitivity was 95% (95% CrI 90% to 97%; 17 studies, 555 rifampicin resistance positives) and pooled specificity was 98% (95% CrI 97% to 99%; 24 studies, 2411 rifampicin resistance negatives). Among 180 specimens with nontuberculous mycobacteria (NTM), Xpert® MTB/RIF was positive in only one specimen that grew NTM (14 studies, 2626 participants).For rifampicin resistance detection, if the pooled accuracy estimates for Xpert® MTB/RIF are applied to a hypothetical cohort of 1000 individuals where 15% of those with symptoms are rifampicin resistant, Xpert® MTB/RIF would correctly identify 143 individuals as rifampicin resistant and miss eight cases, and correctly identify 833 individuals as rifampicin susceptible and misclassify 17 individuals as resistant. Where 5% of those with symptoms are rifampicin resistant, Xpert® MTB/RIF would correctly identify 48 individuals as rifampicin resistant and miss three cases and correctly identify 931 individuals as rifampicin susceptible and misclassify 19 individuals as resistant.
AUTHORS' CONCLUSIONS: In adults thought to have TB, with or without HIV infection, Xpert® MTB/RIF is sensitive and specific. Compared with smear microscopy, Xpert® MTB/RIF substantially increases TB detection among culture-confirmed cases. Xpert® MTB/RIF has higher sensitivity for TB detection in smear-positive than smear-negative patients. Nonetheless, this test may be valuable as an add-on test following smear microscopy in patients previously found to be smear-negative. For rifampicin resistance detection, Xpert® MTB/RIF provides accurate results and can allow rapid initiation of MDR-TB treatment, pending results from conventional culture and DST. The tests are expensive, so current research evaluating the use of Xpert® MTB/RIF in TB programmes in high TB burden settings will help evaluate how this investment may help start treatment promptly and improve outcomes.
准确、快速地检测结核病(TB)及结核耐药性对于改善患者治疗和减少结核病传播至关重要。Xpert® MTB/RIF检测是一项自动化检测,通常可在检测开始后的两小时内同时检测出结核病和利福平耐药性,且实际操作的技术时间最短。世界卫生组织(WHO)于2011年初发布了关于Xpert® MTB/RIF检测的初步建议。2013年1月发表了一篇关于Xpert® MTB/RIF检测对肺结核及利福平耐药性诊断准确性的Cochrane系统评价。我们进行了此次更新的Cochrane系统评价,作为WHO制定该检测使用的更新指南过程的一部分。
评估Xpert® MTB/RIF检测对肺结核(结核病检测)的诊断准确性,其中Xpert® MTB/RIF既作为替代显微镜检查的初始检测,也作为涂片显微镜检查结果为阴性后的补充检测。评估Xpert® MTB/RIF检测对利福平耐药性检测的诊断准确性,其中Xpert® MTB/RIF作为替代基于培养的药物敏感性检测(DST)的初始检测。感兴趣的人群为疑似患有肺结核、利福平耐药或耐多药结核病(MDR-TB)的成年人,无论是否感染HIV。感兴趣的检测地点为中级和基层实验室。后者可能与初级卫生保健机构相关。
我们检索了截至2013年2月7日的以下数据库中任何语言的出版物:Cochrane传染病小组专业注册库;MEDLINE;EMBASE;ISI Web of Knowledge;MEDION;LILACS;BIOSIS;以及SCOPUS。我们还检索了对照试验元注册库(mRCT)和WHO国际临床试验注册平台的检索入口,以识别正在进行的试验。
我们纳入了使用呼吸道标本的随机对照试验、横断面研究和队列研究,这些研究允许提取评估Xpert® MTB/RIF相对于参考标准的数据。我们排除了胃液标本。结核病的参考标准是培养,利福平耐药性的参考标准是基于表型培养的DST。
对于每项研究,两名综述作者使用标准化表格独立提取数据。如有可能,我们按涂片和HIV状态提取亚组数据。我们使用QUADAS-2评估研究质量,并进行荟萃分析以分别估计Xpert® MTB/RIF检测结核病和利福平耐药性的合并敏感性和特异性。对于结核病检测,我们使用双变量随机效应模型进行了大部分分析,并将Xpert® MTB/RIF和涂片显微镜检查相对于培养作为参考标准的敏感性进行了比较。对于利福平耐药性检测,我们分别对敏感性和特异性进行了单变量荟萃分析,以纳入未检测到利福平耐药性的研究。
我们纳入了27项独特的研究(纳入了9项新研究),涉及955名参与者。16项研究(59%)在低收入或中等收入国家进行。对于所有QUADAS-2领域,大多数研究的偏倚风险较低,适用性方面的关注度也较低。作为替代涂片显微镜检查的初始检测,Xpert® MTB/RIF的合并敏感性为89% [95%可信区间(CrI)85%至92%],合并特异性为99%(95% CrI 98%至99%),(22项研究,8998名参与者:2953例确诊结核病,6045例非结核病)。作为涂片显微镜检查结果为阴性后的补充检测,Xpert® MTB/RIF的合并敏感性为67%(95% CrI 60%至74%),合并特异性为99%(95% CrI 98%至99%;21项研究,6950名参与者)。对于涂片阳性、培养阳性的结核病,Xpert® MTB/RIF的合并敏感性为98%(95% CrI 97%至99%;21项研究,1936名参与者)。对于感染HIV的人群,Xpert® MTB/RIF的合并敏感性为79%(95% CrI 70%至86%;7项研究,1789名参与者),对于未感染HIV的人群,为86%(95% CrI 76%至92%;7项研究,1470名参与者)。与涂片显微镜检查的比较与涂片显微镜检查相比