School of Nursing, University of Michigan, 400 North Ingalls Building, Ann Arbor, MI, 48109-5482, USA,
Breast Cancer Res Treat. 2014 Feb;144(1):179-84. doi: 10.1007/s10549-014-2851-8. Epub 2014 Jan 31.
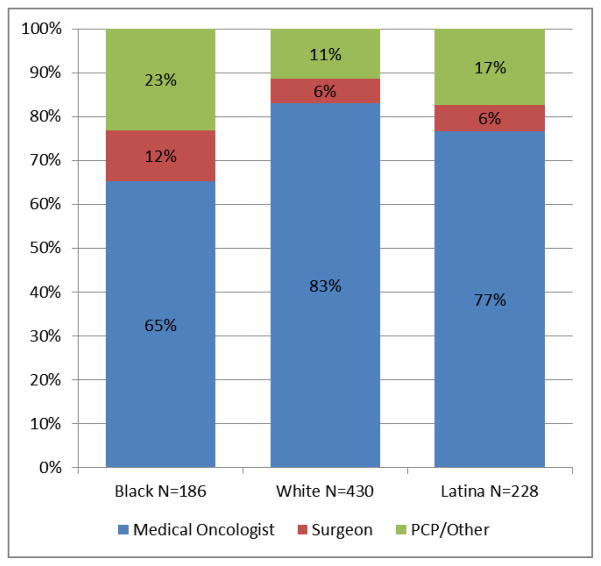
To describe which providers provide breast cancer survivorship care, we conducted a longitudinal survey of nonmetastatic breast cancer patients identified by the SEER registries of Los Angeles and Detroit. Multinomial logistic regression examined the adjusted odds of surgeon compared with a medical oncologist follow-up or primary care provider compared with medical oncologist follow-up, adjusting for age, race/ethnicity, insurance, tumor stage, receipt of chemotherapy, endocrine therapy use, and visit to a medical oncologist at the time of diagnosis. Results were weighted to account for sample selection and nonresponse. 844 women had invasive disease and received chemotherapy or endocrine therapy. 65.2 % reported medical oncologists as their main care provider at 4 years, followed by PCP/other physicians (24.3 %) and surgeons (10.5 %). Black women were more likely to receive their follow-up care from surgeons (OR 2.47, 95 % CI 1.16-5.27) or PCP/other physicians (OR 2.62, 95 % CI 1.47-4.65) than medical oncologists. Latinas were more likely to report PCP/other physician follow-up than medical oncologists (OR 2.33, 95 % CI 1.15-4.73). Compared with privately insured women, Medicaid recipients were more likely to report PCP/other physician follow-up (OR 2.52, 95 % CI 1.24-5.15). Women taking endocrine therapy 4 years after diagnosis were less likely to report surgeons or PCP/other physicians as their primary provider of breast cancer follow-up care. Different survivorship care patterns emerge on race/ethnicity and insurance status. Interventions are needed to inform patients and providers on the recommended sources of breast cancer follow-up.
为了描述哪些提供者提供乳腺癌生存护理,我们对洛杉矶和底特律 SEER 登记处确定的非转移性乳腺癌患者进行了纵向调查。多变量逻辑回归分析了与外科医生相比,与医学肿瘤学家随访或与医学肿瘤学家相比,初级保健提供者随访的调整后优势,调整了年龄、种族/族裔、保险、肿瘤分期、接受化疗、内分泌治疗的使用以及在诊断时是否就诊医学肿瘤学家。结果经过加权处理,以考虑样本选择和无应答。844 名女性患有浸润性疾病并接受化疗或内分泌治疗。65.2%的人报告在 4 年内有医学肿瘤学家作为他们的主要护理提供者,其次是初级保健医生/其他医生(24.3%)和外科医生(10.5%)。黑人女性更有可能接受外科医生(OR 2.47,95%CI 1.16-5.27)或初级保健医生/其他医生(OR 2.62,95%CI 1.47-4.65)的随访护理,而不是医学肿瘤学家。拉丁裔女性更有可能报告初级保健医生/其他医生的随访,而不是医学肿瘤学家(OR 2.33,95%CI 1.15-4.73)。与私人保险女性相比,医疗补助受助人更有可能报告初级保健医生/其他医生的随访(OR 2.52,95%CI 1.24-5.15)。诊断后 4 年服用内分泌治疗的女性更不可能报告外科医生或初级保健医生/其他医生是其乳腺癌随访护理的主要提供者。在种族/族裔和保险状况方面出现了不同的生存护理模式。需要干预措施来告知患者和提供者关于乳腺癌随访的推荐来源。