Bitar Abbas, Selej Mona, Bolad Islam, Lahm Tim
Department of Medicine, Internal Medicine Residency Program, Krannert Institute of Cardiology, Indiana University, Indianapolis, Indiana, United States of America.
Department of Medicine, Division of Pulmonary, Allergy, Critical Care, Occupational and Sleep Medicine, Krannert Institute of Cardiology, Indiana University, Indianapolis, Indiana, United States of America.
PLoS One. 2014 Jan 31;9(1):e87304. doi: 10.1371/journal.pone.0087304. eCollection 2014.
Accurate determination of left ventricular filling pressure is essential for differentiation of pre-capillary pulmonary hypertension (PH) from pulmonary venous hypertension (PVH). Previous data suggest only a poor correlation between left ventricular end-diastolic pressure (LVEDP) and its commonly used surrogate, the pulmonary capillary wedge pressure (PCWP). However, no data exist on the diagnostic accuracy of PCWP in veterans. Furthermore, the effects of age and comorbidities on the PCWP-LVEDP relationship remain unknown.
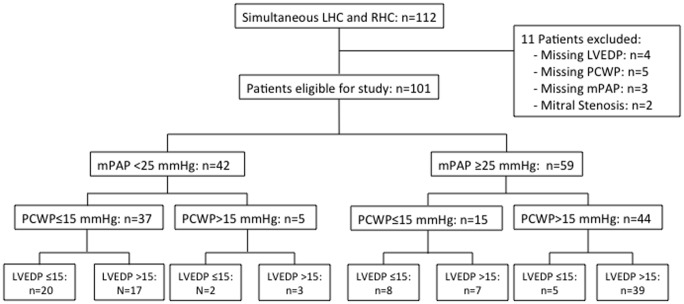
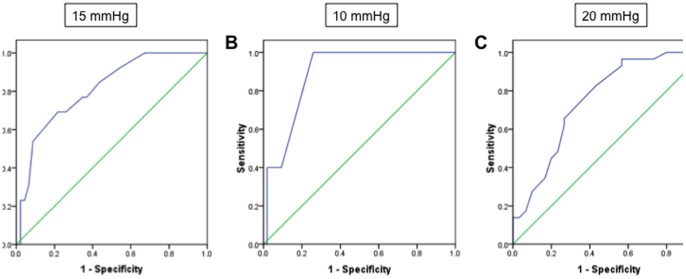
We investigated the PCWP-LVEDP relationship in 101 patients undergoing simultaneous right and left heart catherization at a large VA hospital. PCWP performance was evaluated using correlation and Bland-Altman analyses. Area under Receiver Operating Characteristics curves (AUROC) for PCWP were determined.
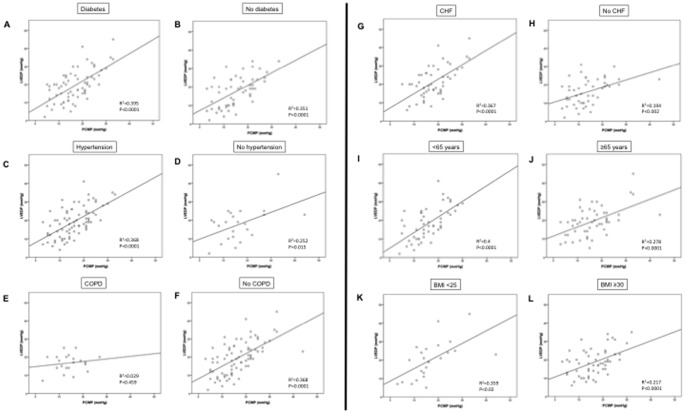
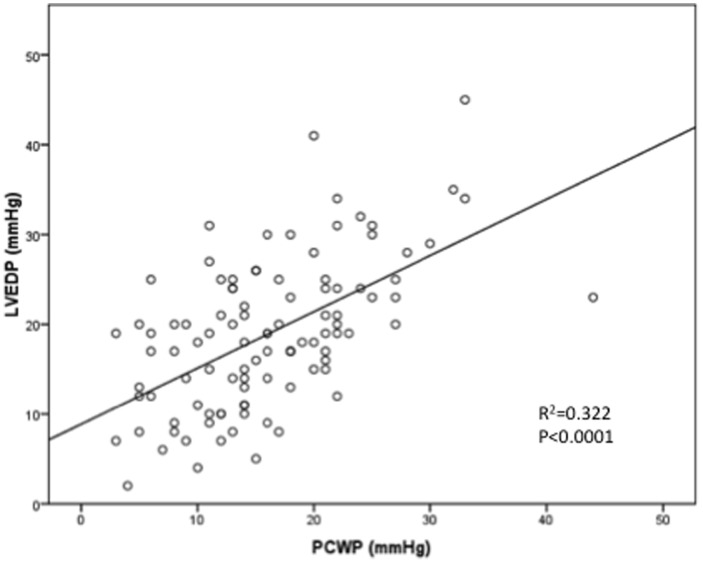
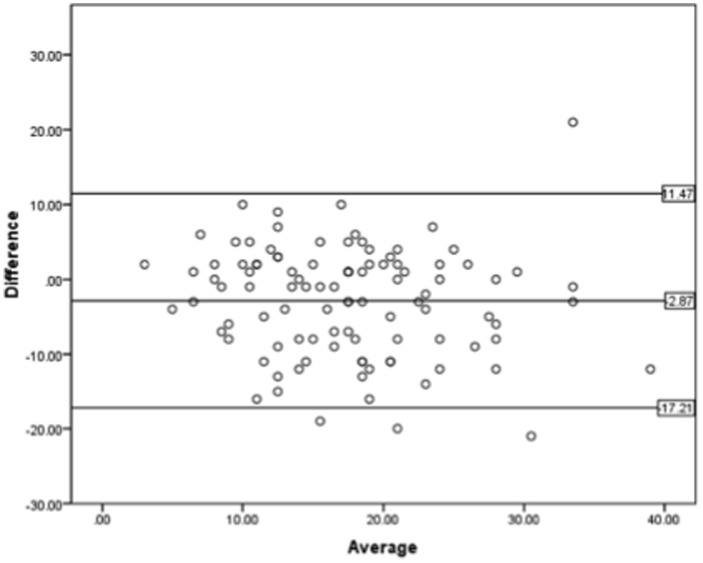
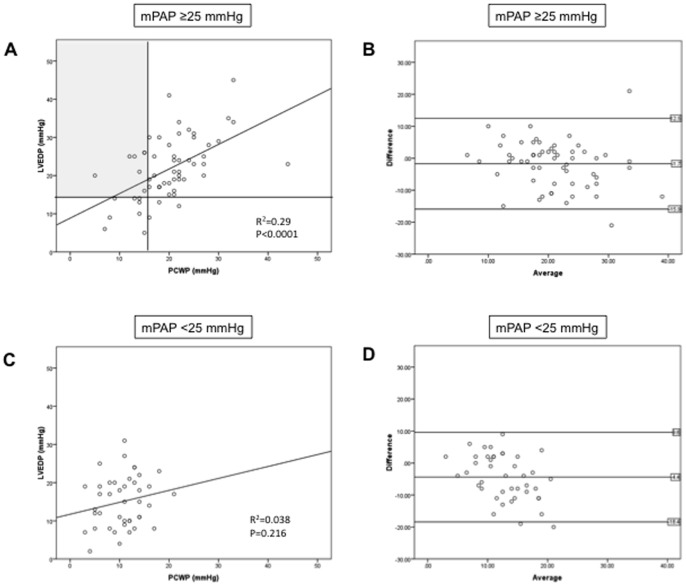
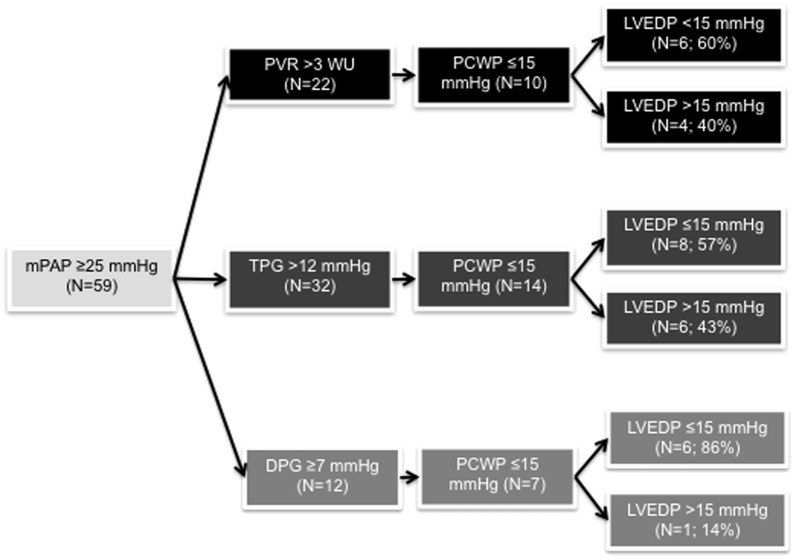
PCWP-LVEDP correlation was moderate (r = 0.57). PCWP-LVEDP calibration was poor (Bland-Altman limits of agreement -17.2 to 11.4 mmHg; mean bias -2.87 mmHg). 59 patients (58.4%) had pulmonary hypertension; 15 (25.4%) of those met pre-capillary PH criteria based on PCWP. However, if LVEDP was used instead of PCWP, 7/15 patients (46.6%) met criteria for PVH rather than pre-capillary PH. When restricting analysis to patients with a mean pulmonary artery pressure of ≥25 mmHg and pulmonary vascular resistance of >3 Wood units (n = 22), 10 patients (45.4%) were classified as pre-capillary PH based on PCWP ≤15 mmHg. However, if LVEDP was used, 4/10 patients (40%) were reclassified as PVH. Among patients with any type of pulmonary hypertension, PCWP discriminated moderately between high and normal LVEDP (AUROC, 0.81; 95%CI 0.69-0.94). PCWP-LVEDP correlation was particularly poor in patients with COPD or obesity.
Reliance on PCWP rather than LVEDP results in misclassification of veterans as having pre-capillary PH rather than PVH in almost 50% of cases. This is clinically relevant, as misclassification may lead to inappropriate therapies and adverse events.
准确测定左心室充盈压对于区分毛细血管前性肺动脉高压(PH)和肺静脉高压(PVH)至关重要。既往数据表明左心室舒张末期压力(LVEDP)与其常用替代指标肺毛细血管楔压(PCWP)之间的相关性较差。然而,尚无关于退伍军人中PCWP诊断准确性的数据。此外,年龄和合并症对PCWP-LVEDP关系的影响仍不清楚。
我们在一家大型退伍军人事务部(VA)医院对101例同时接受右心和左心导管检查的患者的PCWP-LVEDP关系进行了研究。使用相关性分析和Bland-Altman分析评估PCWP的性能。确定PCWP的受试者工作特征曲线下面积(AUROC)。
PCWP与LVEDP的相关性为中等(r = 0.57)。PCWP与LVEDP的校准较差(Bland-Altman一致性界限为-17.2至11.4 mmHg;平均偏差为-2.87 mmHg)。59例患者(58.4%)患有肺动脉高压;其中15例(25.4%)根据PCWP符合毛细血管前性PH标准。然而,如果使用LVEDP而非PCWP,15例患者中有7例(46.6%)符合PVH而非毛细血管前性PH的标准。当将分析限于平均肺动脉压≥25 mmHg且肺血管阻力>3伍德单位的患者(n = 22)时,10例患者(45.4%)根据PCWP≤15 mmHg被分类为毛细血管前性PH。然而,如果使用LVEDP,10例患者中有4例(40%)被重新分类为PVH。在患有任何类型肺动脉高压的患者中,PCWP在高LVEDP和正常LVEDP之间的区分能力中等(AUROC,0.81;95%CI 0.69-0.94)。PCWP与LVEDP的相关性在慢性阻塞性肺疾病(COPD)或肥胖患者中尤其差。
在近50%的病例中,依赖PCWP而非LVEDP会导致退伍军人被错误分类为毛细血管前性PH而非PVH。这具有临床相关性,因为错误分类可能导致不适当的治疗和不良事件。