Rheumatology Allergy and Immunology Division, University of California-San Diego, , La Jolla, California, USA.
Ann Rheum Dis. 2014 Jun;73(6):1000-6. doi: 10.1136/annrheumdis-2013-204741. Epub 2014 Feb 19.
Evaluate ustekinumab, an anti-interleukin (IL)-12 and IL-23 antibody, effects on radiographic progression in psoriatic arthritis (PsA).
We conducted preplanned integrated analyses of combined radiographic data from PSUMMIT-1 and PSUMMIT-2 phase 3, randomised, controlled trials. Patients had active PsA despite prior conventional and/or biologic disease-modifying antirheumatic drugs (≥5/66 swollen, ≥5/68 tender joints, C-reactive protein ≥3.0 mg/L, documented plaque psoriasis). Patients (PSUMMIT-1, n=615; PSUMMIT-2, n=312) were randomised to ustekinumab 45 mg, 90 mg, or placebo, at weeks (wk) 0, 4 and every (q) 12 wks. At wk 16, patients with <5% improvement in tender/swollen joint counts entered blinded early escape. All other placebo patients received ustekinumab 45 mg at wk 24 and wk 28, then q 12 wks. Radiographs of hands/feet at wks 0/24/52 were assessed using PsA-modified van der Heijde-Sharp (vdH-S) scores; combined PSUMMIT-1 and PSUMMIT-2 changes in total vdH-S scores from wk 0 to wk 24 comprised the prespecified primary radiographic analysis. Treatment effects were assessed using analysis of variance on van der Waerden normal scores (factors=treatment, baseline methotrexate usage, and study).
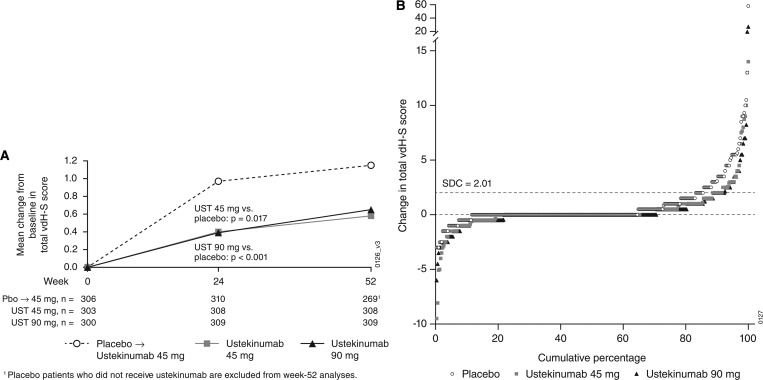
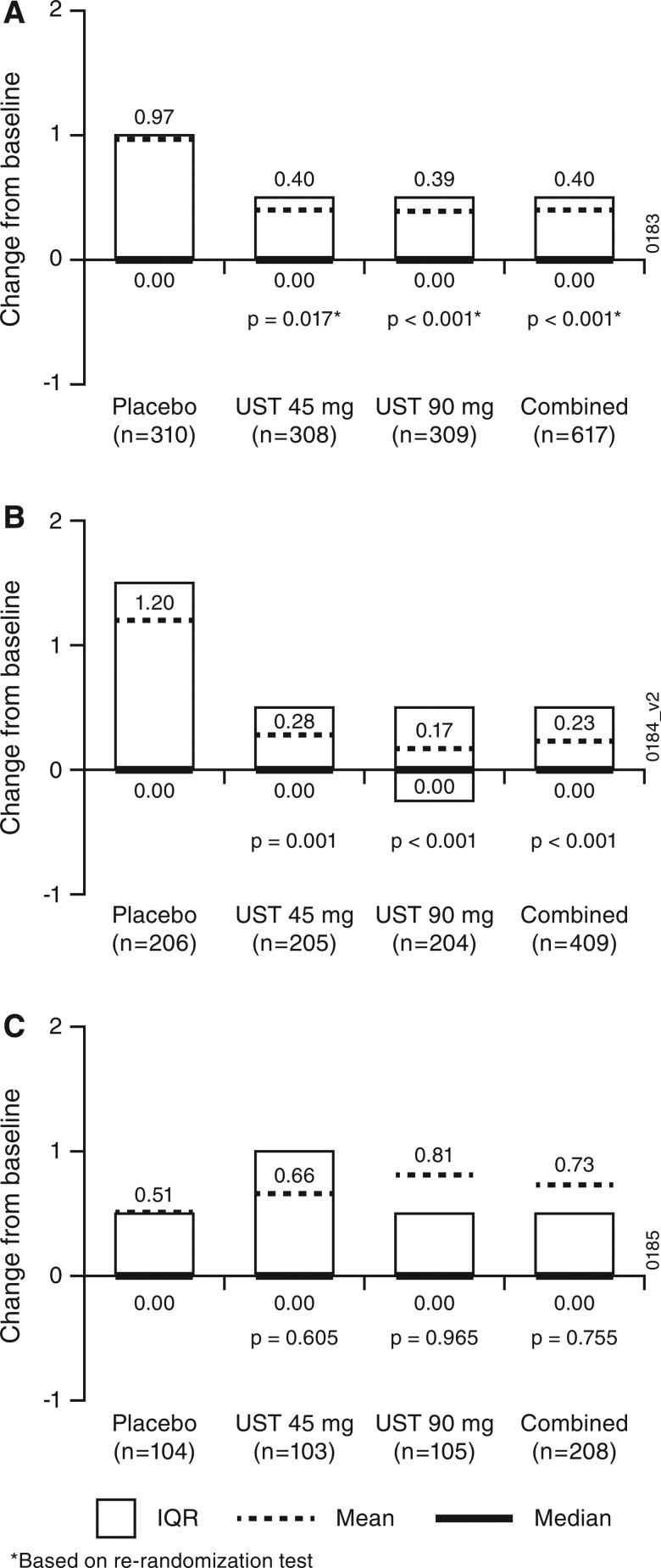
Integrated data analysis results indicated that ustekinumab-treated patients (regardless of dose) demonstrated significantly less radiographic progression at wk 24 than did placebo recipients (wk 0-24 total vdH-S score mean changes: 0.4-combined/individual ustekinumab dose groups, 1.0-placebo; all p<0.02). From wk 24 to wk 52, inhibition of radiographic progression was maintained for ustekinumab-treated patients, and progression was substantially reduced among initial placebo recipients who started ustekinumab at wk 16 or wk 24 (wk 24 - wk 52, total vdH-S score mean change: 0.08).
Ustekinumab 45 and 90 mg treatments significantly inhibited radiographic progression of joint damage in patients with active PsA.
评估乌司奴单抗(一种抗白细胞介素(IL)-12 和 IL-23 的抗体)对银屑病关节炎(PsA)影像学进展的影响。
我们对 PSUMMIT-1 和 PSUMMIT-2 两项 3 期、随机、对照临床试验的联合影像学数据进行了预设的综合分析。这些患者尽管接受了先前的常规和/或生物改善病情抗风湿药物(≥5/66 个肿胀关节,≥5/68 个触痛关节,C 反应蛋白≥3.0mg/L,有记录的斑块型银屑病)治疗,但仍处于活动性 PsA 中。患者(PSUMMIT-1,n=615;PSUMMIT-2,n=312)按 0、4 和每 12 周(q)的方案随机接受乌司奴单抗 45mg、90mg 或安慰剂治疗。在第 16 周,对压痛/肿胀关节计数改善<5%的患者进行盲法早期逃逸。所有其他安慰剂患者在第 24 周和第 28 周接受乌司奴单抗 45mg 治疗,然后每 12 周治疗一次。在第 0、24 和 52 周时,采用改良的 PsA van der Heijde-Sharp(vdH-S)评分评估手部/足部 X 线片;0 至 24 周时的总 vdH-S 评分变化构成了预设的主要影像学分析。采用方差分析(因子=治疗、基线甲氨蝶呤使用情况和研究)评估治疗效果。
综合数据分析结果表明,与安慰剂组相比,乌司奴单抗治疗患者(无论剂量如何)在第 24 周时的影像学进展明显减少(第 0-24 周的总 vdH-S 评分变化:联合/个体乌司奴单抗剂量组为 0.4,安慰剂组为 1.0;所有 p<0.02)。从第 24 周到第 52 周,乌司奴单抗治疗患者的影像学进展抑制得以维持,而在第 16 周或第 24 周开始接受乌司奴单抗治疗的初始安慰剂组患者的进展明显减少(第 24-52 周,总 vdH-S 评分变化:0.08)。
乌司奴单抗 45mg 和 90mg 治疗可显著抑制活动性 PsA 患者的关节损伤影像学进展。