Fudman David I, Lightdale Charles J, Poneros John M, Ginsberg Gregory G, Falk Gary W, Demarshall Maureen, Gupta Milli, Iyer Prasad G, Lutzke Lori, Wang Kenneth K, Abrams Julian A
Division of Digestive and Liver Diseases, Columbia University Medical Center, New York, New York, USA.
Division of Gastroenterology, University of Pennsylvania Perelman School of Medicine, Philadelphia, Pennsylvania, USA.
Gastrointest Endosc. 2014 Jul;80(1):71-7. doi: 10.1016/j.gie.2014.01.007. Epub 2014 Feb 22.
Radiofrequency ablation (RFA) has become an accepted form of endoscopic treatment for Barrett's esophagus (BE), yet reported response rates are variable. There are no accepted quality measures for performing RFA, and provider-level characteristics may influence RFA outcomes.
To determine whether endoscopist RFA volume is associated with rates of complete remission of intestinal metaplasia (CRIM) after RFA in patients with BE.
Retrospective analysis of longitudinal data.
Three tertiary-care medical centers.
Patients with BE treated with RFA.
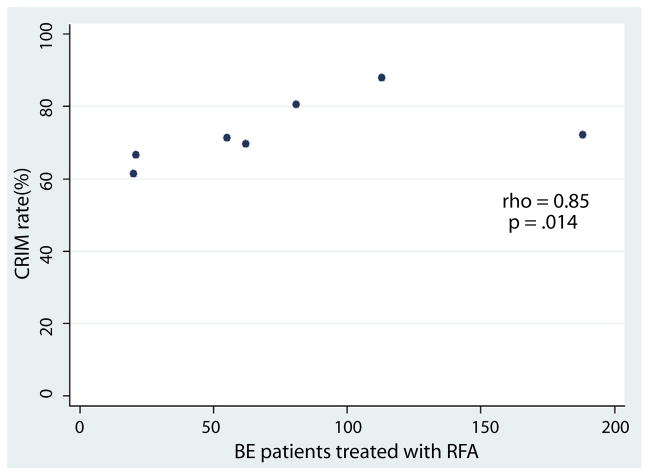
For each endoscopist, we recorded RFA volume, defined as the number of unique patients treated as well as corresponding CRIM rates. We calculated a Spearman correlation coefficient relating these 2 measures.
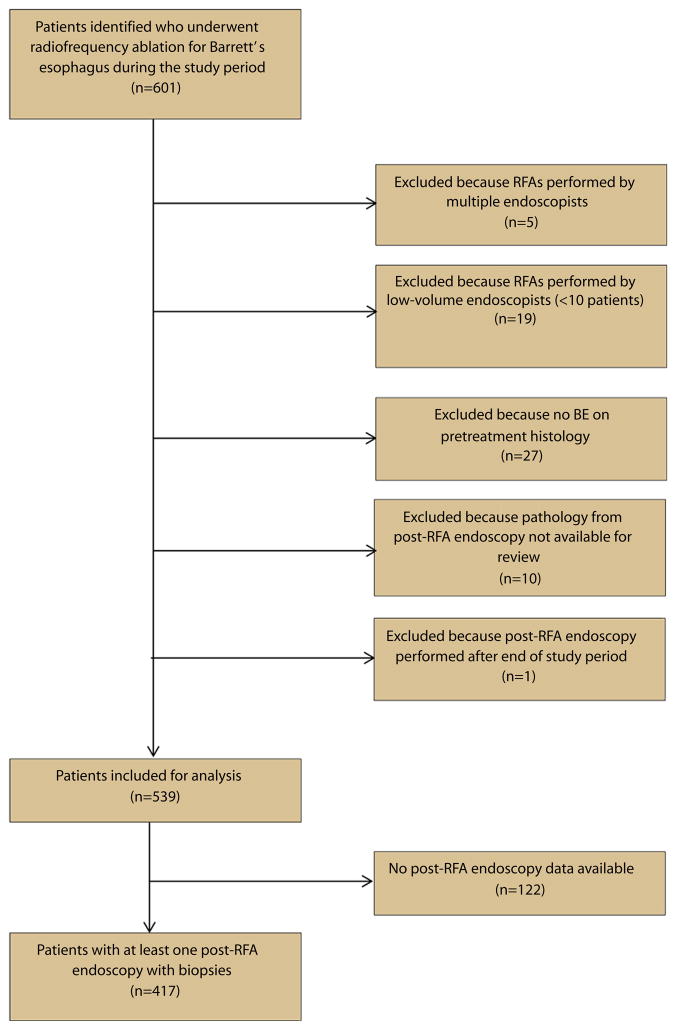
We identified 417 patients with BE treated with RFA who had at least 1 post-RFA endoscopy with biopsies. A total of 73% of the cases had pretreatment histology of high-grade dysplasia or adenocarcinoma. The procedures were performed by 7 endoscopists, who had a median RFA volume of 62 patients (range 20-188). The overall CRIM rate was 75.3% (provider range 62%-88%). The correlation between endoscopist RFA volume and CRIM rate was strong and significant (rho = 0.85; P = .014). In multivariable analysis, higher RFA volume was significantly associated with CRIM (P for trend .04).
Referral setting may limit generalizability. Limited number of endoscopists analyzed.
Endoscopist RFA volume correlates with rates of successful BE eradication. Further studies are required to confirm these findings and to determine whether RFA volume is a valid predictor of treatment outcomes in BE.
射频消融术(RFA)已成为治疗巴雷特食管(BE)的一种公认的内镜治疗方式,但报告的缓解率各不相同。目前尚无公认的RFA质量衡量标准,医疗服务提供者层面的特征可能会影响RFA的治疗效果。
确定内镜医师进行RFA的例数是否与BE患者RFA术后肠化生完全缓解率(CRIM)相关。
对纵向数据进行回顾性分析。
三个三级医疗中心。
接受RFA治疗的BE患者。
RFA
对于每位内镜医师,我们记录了RFA例数,定义为接受治疗的独特患者数量以及相应的CRIM率。我们计算了这两个指标之间的Spearman相关系数。
我们确定了417例接受RFA治疗的BE患者,这些患者至少接受了1次RFA术后内镜活检。共有73%的病例术前组织学检查为高级别异型增生或腺癌。这些手术由7位内镜医师进行,他们的RFA例数中位数为62例患者(范围为20 - 188例)。总体CRIM率为75.3%(医疗服务提供者范围为62% - 88%)。内镜医师RFA例数与CRIM率之间的相关性很强且具有统计学意义(rho = 0.85;P = 0.014)。在多变量分析中,较高的RFA例数与CRIM显著相关(趋势P值为0.04)。
转诊环境可能会限制研究结果的普遍性。分析的内镜医师数量有限。
内镜医师的RFA例数与BE成功根除率相关。需要进一步研究来证实这些发现,并确定RFA例数是否是BE治疗效果的有效预测指标。