Marks Michael P, Lansberg Maarten G, Mlynash Michael, Olivot Jean-Marc, Straka Matus, Kemp Stephanie, McTaggart Ryan, Inoue Manabu, Zaharchuk Greg, Bammer Roland, Albers Gregory W
From Stanford Stroke Center, Stanford University School of Medicine, Palo Alto, CA.
Stroke. 2014 Apr;45(4):1035-9. doi: 10.1161/STROKEAHA.113.004085. Epub 2014 Feb 25.
Our aim was to determine the relationships between angiographic collaterals and diffusion/perfusion findings, subsequent infarct growth, and clinical outcome in patients undergoing endovascular therapy for ischemic stroke.
Sixty patients with a thrombolysis in cerebral infarction (TICI) score of 0 or 1 and internal carotid artery/M1 occlusion at baseline were evaluated. A blinded reader assigned a collateral score using a previous 5-point scale, from 0 (no collateral flow) to 4 (complete/rapid collaterals to the entire ischemic territory). The analysis was dichotomized to poor flow (0-2) versus good flow (3-4). Collateral score was correlated with baseline National Institutes of Health Stroke Scale, diffusion-weighted imaging volume, perfusion-weighted imaging volume (Tmax ≥6 seconds), TICI reperfusion, infarct growth, and modified Rankin Scale score at day 90.
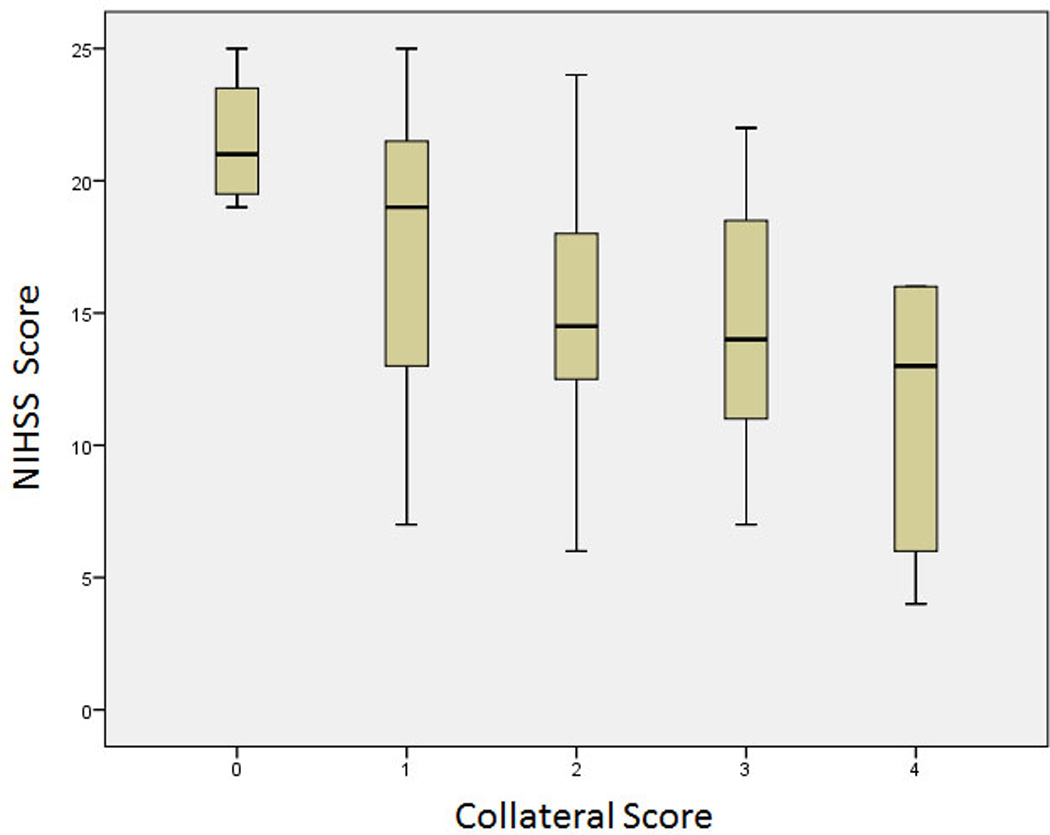
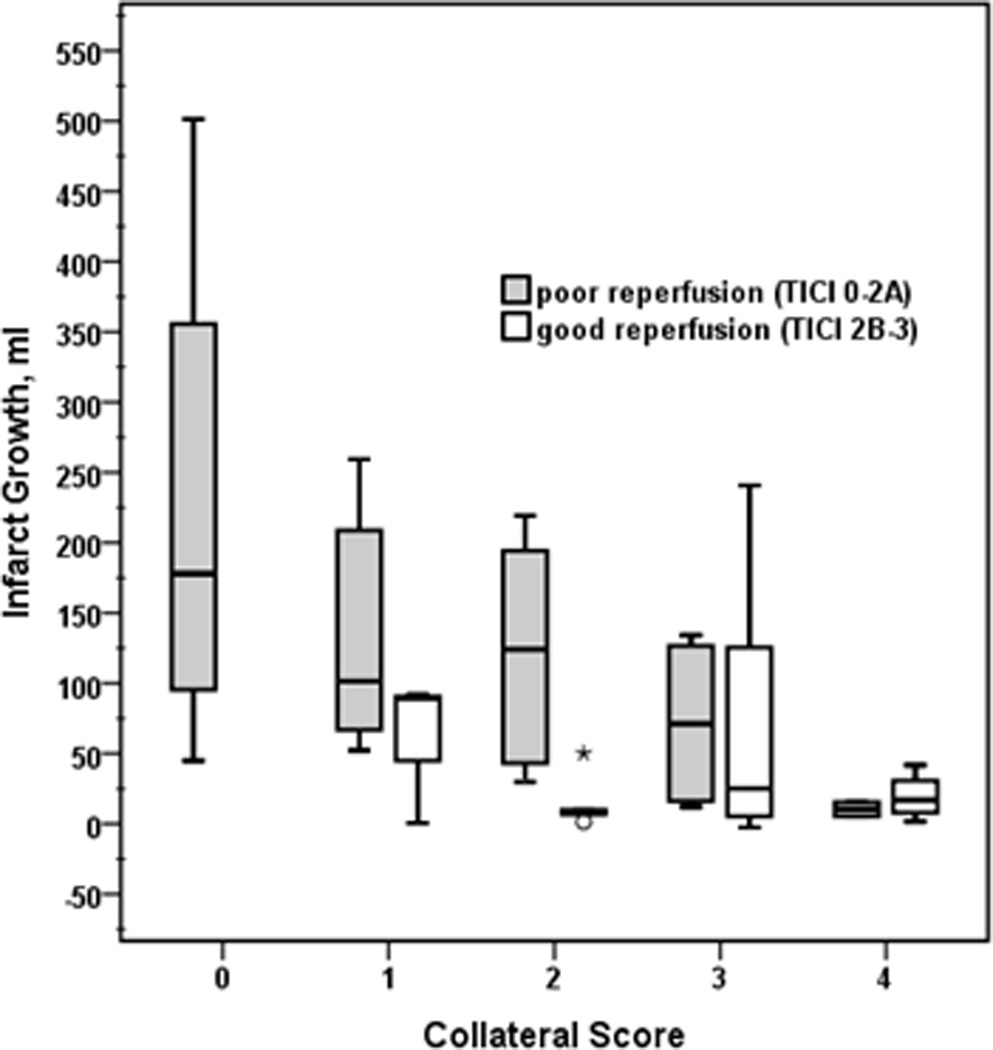
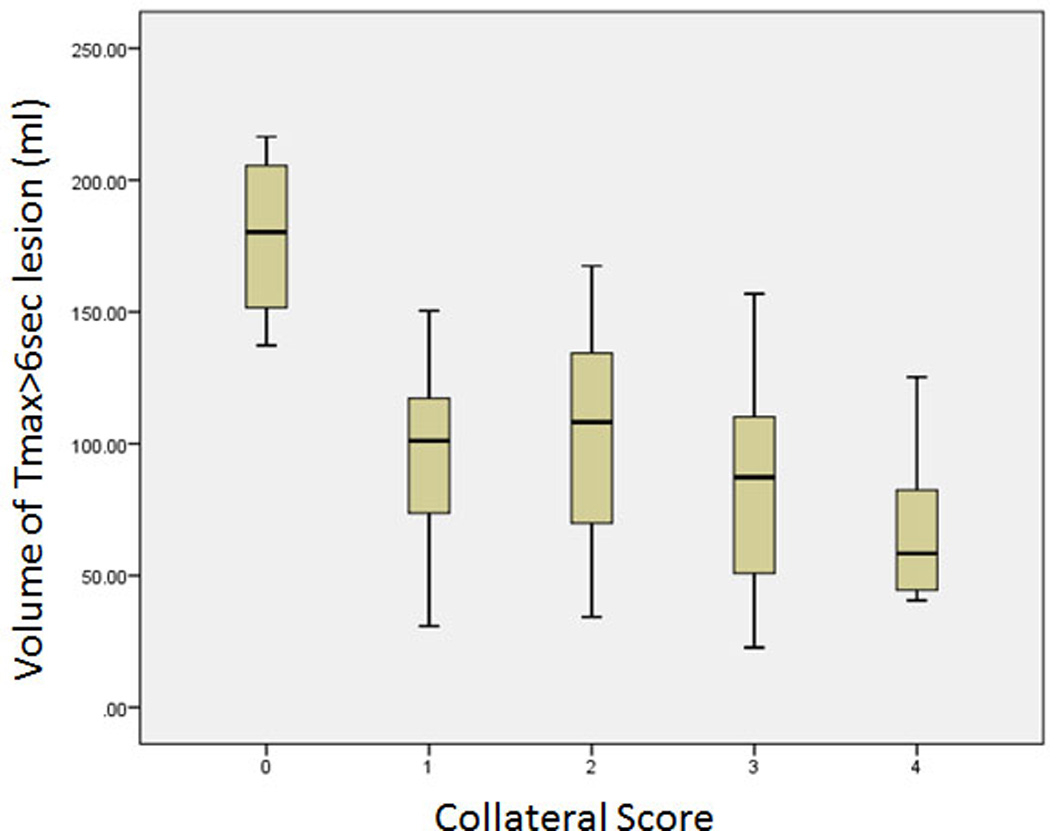
Collateral score correlated with baseline National Institutes of Health Stroke Scale (P=0.002) and median volume of tissue at Tmax ≥6 seconds (P=0.009). Twenty-nine percent of patients with poor collateral flow had TICI 2B-3 reperfusion versus 65.5% with good flow (P=0.009). Patients with poor collaterals who reperfused (TICI 2B-3) were more likely to have a good functional outcome (modified Rankin Scale score 0-2 at 90 days) compared with patients who did not reperfuse (odds ratio, 12; 95% confidence interval, 1.6-98). There was no difference in the rate of good functional outcome after reperfusion in patients with poor collaterals versus good collaterals (P=1.0). Patients with poor reperfusion (TICI 0-2a) showed a trend toward greater infarct growth if they had poor collaterals versus good collaterals (P=0.06).
Collaterals correlate with baseline National Institutes of Health Stroke Scale, perfusion-weighted imaging volume, and good reperfusion. However, target mismatch patients who reperfuse seem to have favorable outcomes at a similar rate, irrespective of the collateral score.
http://www.clinicaltrials.gov. Unique identifier: NCT01349946.
我们的目的是确定接受缺血性卒中血管内治疗的患者血管造影侧支循环与弥散/灌注结果、随后的梗死灶扩大及临床结局之间的关系。
对60例基线时脑梗死溶栓(TICI)评分0或1且颈内动脉/M1闭塞的患者进行评估。一名盲法阅片者采用先前的5分制对侧支循环进行评分,从0分(无侧支血流)到4分(向整个缺血区域的完全/快速侧支循环)。分析分为血流差(0 - 2分)与血流好(3 - 4分)两组。侧支循环评分与基线美国国立卫生研究院卒中量表、弥散加权成像体积、灌注加权成像体积(Tmax≥6秒)、TICI再灌注、梗死灶扩大及90天时改良Rankin量表评分相关。
侧支循环评分与基线美国国立卫生研究院卒中量表(P = 0.002)及Tmax≥6秒时的组织中位数体积(P = 0.009)相关。侧支血流差的患者中29%实现了TICI 2B - 3级再灌注,而侧支血流好的患者中这一比例为65.5%(P = 0.009)。与未实现再灌注的患者相比,实现再灌注(TICI 2B - 3)的侧支循环差的患者更有可能获得良好的功能结局(90天时改良Rankin量表评分为0 - 2分)(优势比,12;95%置信区间,1.6 - 98)。侧支循环差的患者与侧支循环好的患者再灌注后良好功能结局的发生率无差异(P = 1.0)。再灌注差(TICI 0 - 2a)的患者中,侧支循环差者梗死灶扩大的趋势大于侧支循环好者(P = 0.06)。
侧支循环与基线美国国立卫生研究院卒中量表、灌注加权成像体积及良好的再灌注相关。然而,实现再灌注的目标不匹配患者似乎无论侧支循环评分如何都有相似比例的良好结局。