Kaiser Thorsten, Kinny-Köster Benedict, Bartels Michael, Parthaune Tanja, Schmidt Michael, Thiery Joachim
Institute of Laboratory Medicine, Clinical Chemistry and Molecular Diagnostics, University Hospital Leipzig, Leipzig, Germany.
Department of Visceral, Vascular, Thoracic and Transplant Surgery, University Hospital of Leipzig, Leipzig, Germany.
PLoS One. 2014 Feb 27;9(2):e90015. doi: 10.1371/journal.pone.0090015. eCollection 2014.
The model for end-stage liver disease (MELD) score is used in many countries to prioritize organ allocation for the majority of patients who require orthotopic liver transplantation. This score is calculated based on the following laboratory parameters: creatinine, bilirubin and the international normalized ratio (INR). Consequently, high measurement accuracy is essential for equitable and fair organ allocation. For serum creatinine measurements, the Jaffé method and enzymatic detection are well-established routine diagnostic tests.
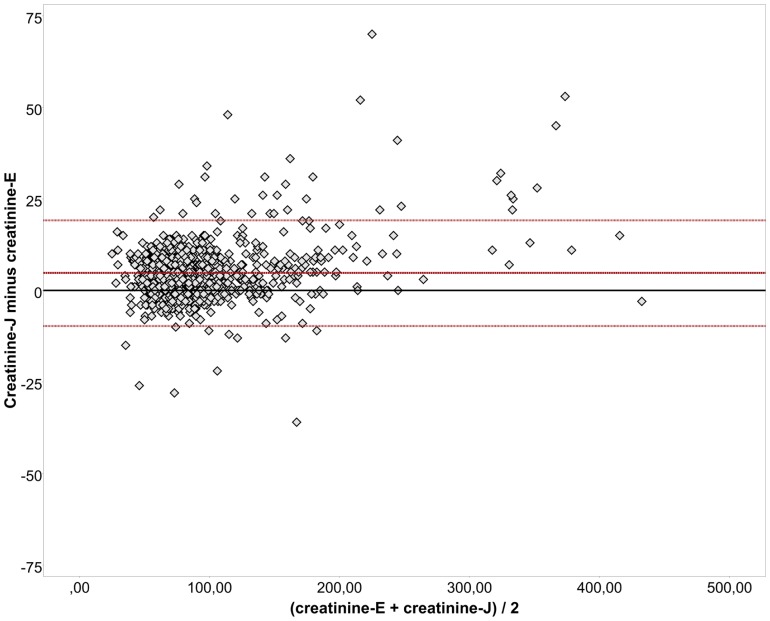
A total of 1,013 samples from 445 patients on the waiting list or in evaluation for liver transplantation were measured using both creatinine methods from November 2012 to September 2013 at the university hospital Leipzig, Germany. The measurements were performed in parallel according to the manufacturer's instructions after the samples arrived at the institute of laboratory medicine. Patients who had required renal replacement therapy twice in the previous week were excluded from analyses.
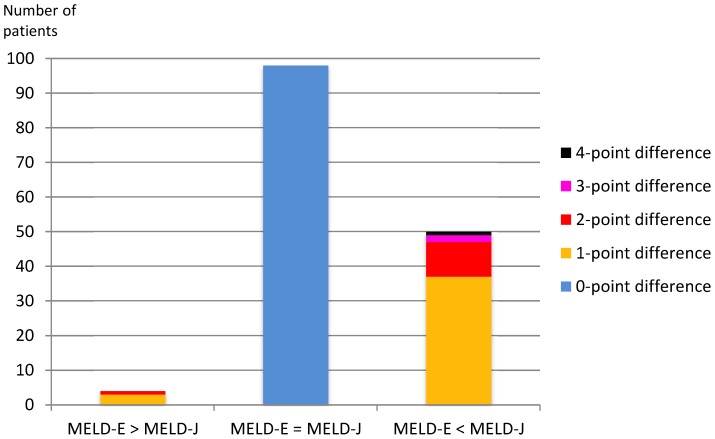
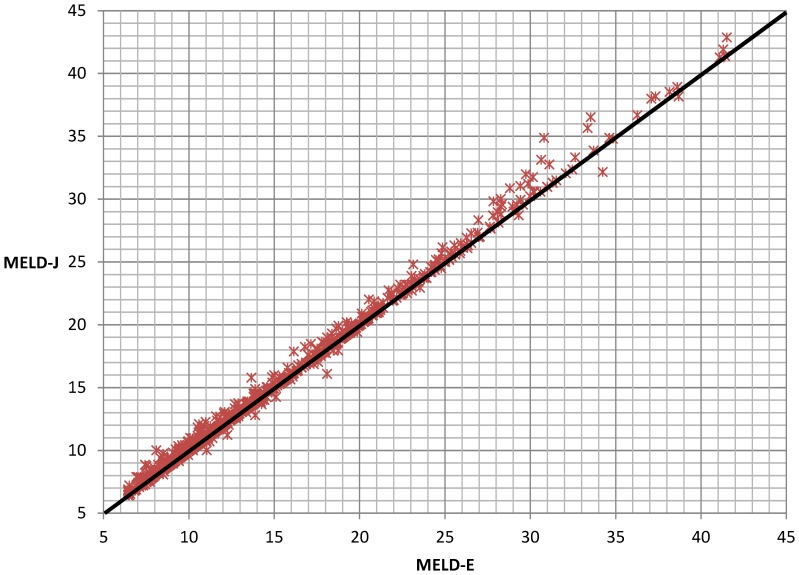
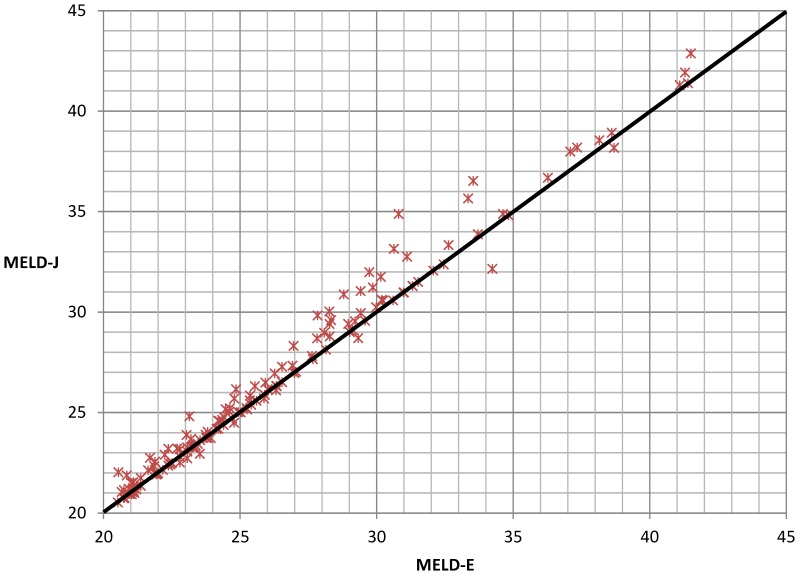
Despite the good correlation between the results of both creatinine quantification methods, relevant differences were observed, which led to different MELD scores. The Jaffé measurement led to greater MELD score in 163/1,013 (16.1%) samples with differences of up to 4 points in one patient, whereas differences of up to 2 points were identified in 15/1,013 (1.5%) samples using the enzymatic assay. Overall, 50/152 (32.9%) patients with MELD scores >20 had higher scores when the Jaffé method was used.
Using the Jaffé method to measure creatinine levels in samples from patients who require liver transplantation may lead to a systematic preference in organ allocation. In this study, the differences were particularly pronounced in samples with MELD scores >20, which has clinical relevance in the context of urgency of transplantation. These data suggest that official recommendations are needed to determine which laboratory diagnostic methods should be used when calculating MELD scores.
终末期肝病模型(MELD)评分在许多国家被用于为大多数需要原位肝移植的患者确定器官分配的优先顺序。该评分基于以下实验室参数计算得出:肌酐、胆红素和国际标准化比值(INR)。因此,高测量准确性对于公平公正的器官分配至关重要。对于血清肌酐测量,Jaffé法和酶法检测是成熟的常规诊断测试。
2012年11月至2013年9月期间,在德国莱比锡大学医院,使用两种肌酐检测方法对445名等待肝移植或正在接受肝移植评估的患者的1013份样本进行了检测。样本抵达检验医学研究所后,按照制造商的说明并行进行检测。排除前一周需要进行两次肾脏替代治疗的患者进行分析。
尽管两种肌酐定量方法的结果之间具有良好的相关性,但仍观察到了显著差异,这导致了不同的MELD评分。Jaffé法测量使163/1013(16.1%)的样本MELD评分更高,其中一名患者的差异高达4分,而使用酶法检测时,15/1013(1.5%)的样本差异高达2分。总体而言,使用Jaffé法时,MELD评分>20的患者中有50/152(32.9%)的评分更高。
使用Jaffé法测量需要肝移植患者样本中的肌酐水平可能会导致器官分配中的系统性偏好。在本研究中,差异在MELD评分>20的样本中尤为明显,这在移植紧迫性的背景下具有临床相关性。这些数据表明,需要官方建议来确定在计算MELD评分时应使用哪种实验室诊断方法。