Wingfield Tom, Schumacher Samuel G, Sandhu Gurjinder, Tovar Marco A, Zevallos Karine, Baldwin Matthew R, Montoya Rosario, Ramos Eric S, Jongkaewwattana Chulanee, Lewis James J, Gilman Robert H, Friedland Jon S, Evans Carlton A
IFHAD: Innovation For Health and Development, United Kingdom Infectious Diseases and Immunity, Imperial College London Wellcome Trust Imperial College Centre for Global Health Research, London The Monsall Infectious Diseases Unit, North Manchester General Hospital, Manchester.
IFHAD: Innovation For Health and Development, United Kingdom Laboratorio de Investigación y Desarrollo, Universidad Peruana Cayetano Heredia, Perú
J Infect Dis. 2014 Sep 1;210(5):774-83. doi: 10.1093/infdis/jiu121. Epub 2014 Mar 4.
Unlike other respiratory infections, tuberculosis diagnoses increase in summer. We performed an ecological analysis of this paradoxical seasonality in a Peruvian shantytown over 4 years.
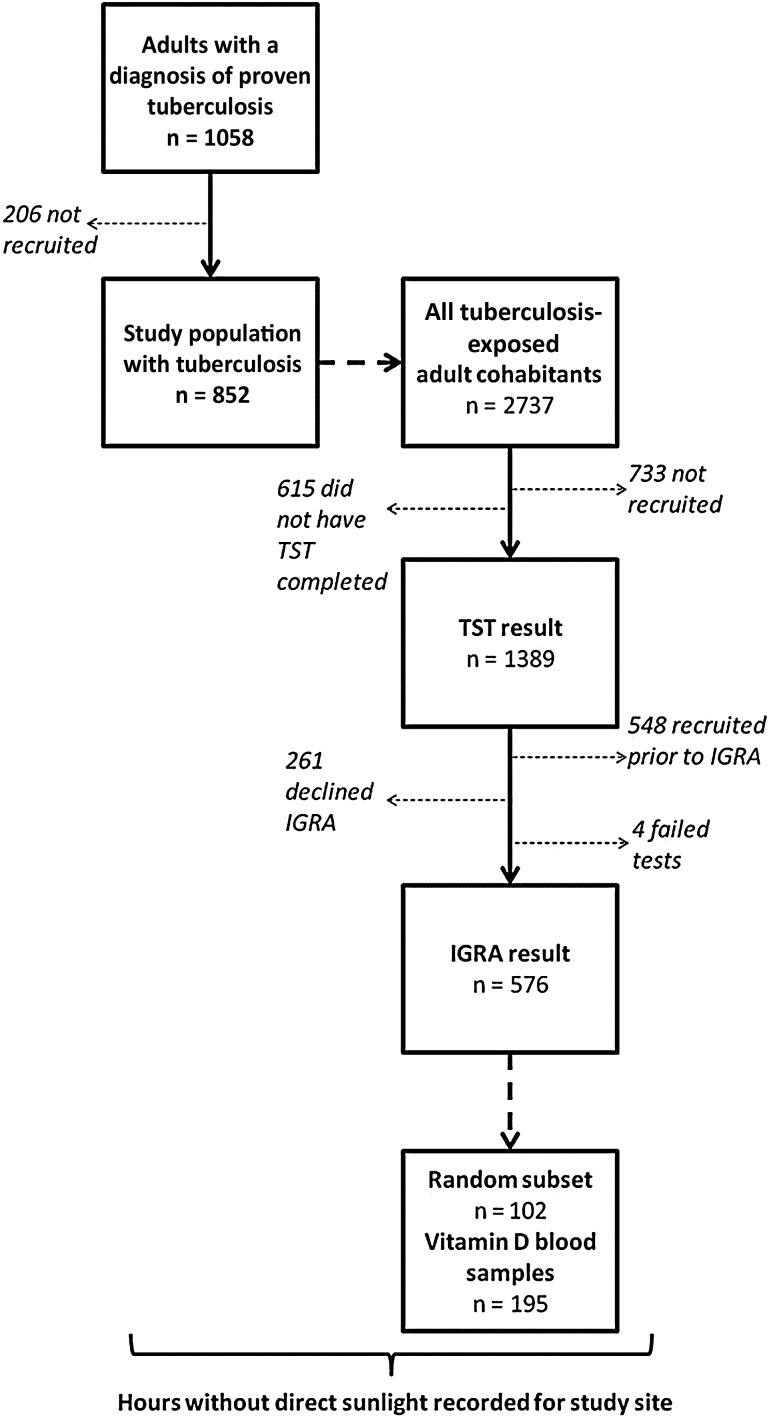
Tuberculosis symptom-onset and diagnosis dates were recorded for 852 patients. Their tuberculosis-exposed cohabitants were tested for tuberculosis infection with the tuberculin skin test (n = 1389) and QuantiFERON assay (n = 576) and vitamin D concentrations (n = 195) quantified from randomly selected cohabitants. Crowding was calculated for all tuberculosis-affected households and daily sunlight records obtained.
Fifty-seven percent of vitamin D measurements revealed deficiency (<50 nmol/L). Risk of deficiency was increased 2.0-fold by female sex (P < .001) and 1.4-fold by winter (P < .05). During the weeks following peak crowding and trough sunlight, there was a midwinter peak in vitamin D deficiency (P < .02). Peak vitamin D deficiency was followed 6 weeks later by a late-winter peak in tuberculin skin test positivity and 12 weeks after that by an early-summer peak in QuantiFERON positivity (both P < .04). Twelve weeks after peak QuantiFERON positivity, there was a midsummer peak in tuberculosis symptom onset (P < .05) followed after 3 weeks by a late-summer peak in tuberculosis diagnoses (P < .001).
The intervals from midwinter peak crowding and trough sunlight to sequential peaks in vitamin D deficiency, tuberculosis infection, symptom onset, and diagnosis may explain the enigmatic late-summer peak in tuberculosis.
与其他呼吸道感染不同,肺结核的诊断在夏季会增加。我们对秘鲁一个棚户区4年中的这种矛盾的季节性进行了生态分析。
记录了852例患者的肺结核症状出现和诊断日期。对其接触过肺结核的同居者进行结核菌素皮肤试验(n = 1389)和全血γ干扰素释放试验(n = 576)以检测结核感染,并对随机选择的同居者定量测定维生素D浓度(n = 195)。计算了所有受肺结核影响家庭的拥挤程度,并获取了每日阳光照射记录。
57%的维生素D测量结果显示缺乏(<50 nmol/L)。女性维生素D缺乏风险增加2.0倍(P <.001),冬季增加1.4倍(P <.05)。在拥挤高峰和阳光照射低谷后的几周内,维生素D缺乏出现了冬季中期高峰(P <.02)。维生素D缺乏高峰6周后,结核菌素皮肤试验阳性出现了冬末高峰,再过12周,全血γ干扰素释放试验阳性出现了初夏高峰(均P <.04)。全血γ干扰素释放试验阳性高峰12周后,肺结核症状出现了仲夏高峰(P <.05),3周后肺结核诊断出现了夏末高峰(P <.001)。
从冬季中期拥挤高峰和阳光照射低谷到维生素D缺乏、结核感染、症状出现和诊断的相继高峰之间的时间间隔,可能解释了肺结核在夏末出现的神秘高峰。