Li Jonathan Z, Chapman Brad, Charlebois Patrick, Hofmann Oliver, Weiner Brian, Porter Alyssa J, Samuel Reshmi, Vardhanabhuti Saran, Zheng Lu, Eron Joseph, Taiwo Babafemi, Zody Michael C, Henn Matthew R, Kuritzkes Daniel R, Hide Winston, Wilson Cara C, Berzins Baiba I, Acosta Edward P, Bastow Barbara, Kim Peter S, Read Sarah W, Janik Jennifer, Meres Debra S, Lederman Michael M, Mong-Kryspin Lori, Shaw Karl E, Zimmerman Louis G, Leavitt Randi, De La Rosa Guy, Jennings Amy
Division of Infectious Diseases, Brigham and Women's Hospital, Harvard Medical School, Boston, Massachusetts, United States of America.
Harvard School of Public Health, Boston, Massachusetts, United States of America.
PLoS One. 2014 Mar 6;9(3):e90485. doi: 10.1371/journal.pone.0090485. eCollection 2014.
The impact of raltegravir-resistant HIV-1 minority variants (MVs) on raltegravir treatment failure is unknown. Illumina sequencing offers greater throughput than 454, but sequence analysis tools for viral sequencing are needed. We evaluated Illumina and 454 for the detection of HIV-1 raltegravir-resistant MVs.
A5262 was a single-arm study of raltegravir and darunavir/ritonavir in treatment-naïve patients. Pre-treatment plasma was obtained from 5 participants with raltegravir resistance at the time of virologic failure. A control library was created by pooling integrase clones at predefined proportions. Multiplexed sequencing was performed with Illumina and 454 platforms at comparable costs. Illumina sequence analysis was performed with the novel snp-assess tool and 454 sequencing was analyzed with V-Phaser.
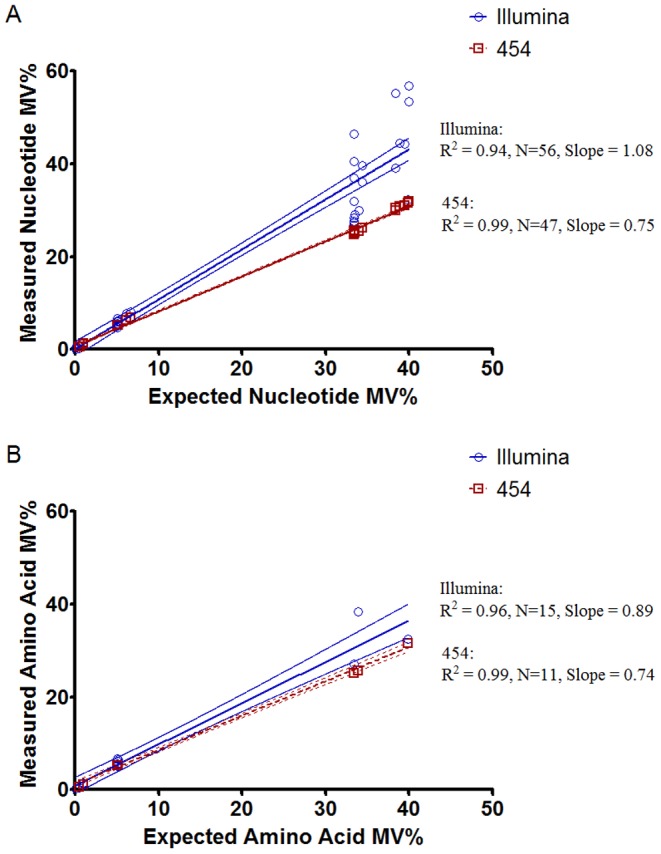
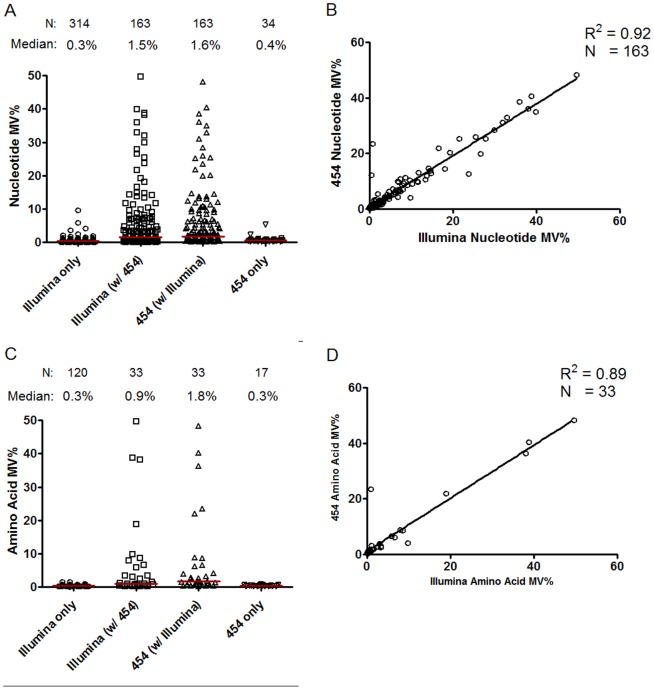
Illumina sequencing resulted in significantly higher sequence coverage and a 0.095% limit of detection. Illumina accurately detected all MVs in the control library at ≥0.5% and 7/10 MVs expected at 0.1%. 454 sequencing failed to detect any MVs at 0.1% with 5 false positive calls. For MVs detected in the patient samples by both 454 and Illumina, the correlation in the detected variant frequencies was high (R2 = 0.92, P<0.001). Illumina sequencing detected 2.4-fold greater nucleotide MVs and 2.9-fold greater amino acid MVs compared to 454. The only raltegravir-resistant MV detected was an E138K mutation in one participant by Illumina sequencing, but not by 454.
In participants of A5262 with raltegravir resistance at virologic failure, baseline raltegravir-resistant MVs were rarely detected. At comparable costs to 454 sequencing, Illumina demonstrated greater depth of coverage, increased sensitivity for detecting HIV MVs, and fewer false positive variant calls.
具有雷特格韦耐药性的HIV-1少数变异株(MVs)对雷特格韦治疗失败的影响尚不清楚。Illumina测序比454测序通量更高,但需要用于病毒测序的序列分析工具。我们评估了Illumina和454在检测HIV-1雷特格韦耐药MVs方面的性能。
A5262是一项针对初治患者使用雷特格韦和达芦那韦/利托那韦的单臂研究。在病毒学失败时,从5名具有雷特格韦耐药性的参与者中获取治疗前血浆。通过以预定比例混合整合酶克隆创建对照文库。使用Illumina和454平台以相当的成本进行多重测序。使用新型snp-assess工具进行Illumina序列分析,使用V-Phaser分析454测序结果。
Illumina测序产生了显著更高的序列覆盖率和0.095%的检测限。Illumina准确检测到对照文库中所有≥0.5%的MVs以及预期的10个MVs中的7个(0.1%水平)。454测序未能检测到任何0.1%水平的MVs,出现了5例假阳性结果。对于454和Illumina在患者样本中均检测到的MVs,检测到的变异频率之间的相关性很高(R2 = 0.92,P<0.001)。与454相比,Illumina测序检测到的核苷酸MVs多2.4倍,氨基酸MVs多2.9倍。唯一检测到的雷特格韦耐药MV是一名参与者中通过Illumina测序发现的E138K突变,而454测序未检测到。
在A5262中病毒学失败时具有雷特格韦耐药性的参与者中,很少检测到基线雷特格韦耐药MVs。与454测序成本相当的情况下,Illumina显示出更高的覆盖深度、更高的检测HIV MVs的灵敏度以及更少的假阳性变异结果。