Yun Huifeng, Xie Fenglong, Delzell Elizabeth, Chen Lang, Levitan Emily B, Lewis James D, Saag Kenneth G, Beukelman Timothy, Winthrop Kevin, Baddley John W, Curtis Jeffrey R
Department of Epidemiology, University of Alabama at Birmingham, Birmingham, Alabama, USA Division of Clinical Immunology and Rheumatology, University of Alabama at Birmingham, Birmingham, Alabama, USA.
Division of Clinical Immunology and Rheumatology, University of Alabama at Birmingham, Birmingham, Alabama, USA.
Ann Rheum Dis. 2015 Jun;74(6):1065-71. doi: 10.1136/annrheumdis-2013-204011. Epub 2014 Mar 7.
The risk of subsequent infections in rheumatoid arthritis (RA) patients who receive biologic therapy after a serious infection is unclear.
To compare the subsequent risk of hospitalised infections associated with specific biologic agents among RA patients previously hospitalised for infection while receiving anti-tumour necrosis factor (anti-TNF) therapy.
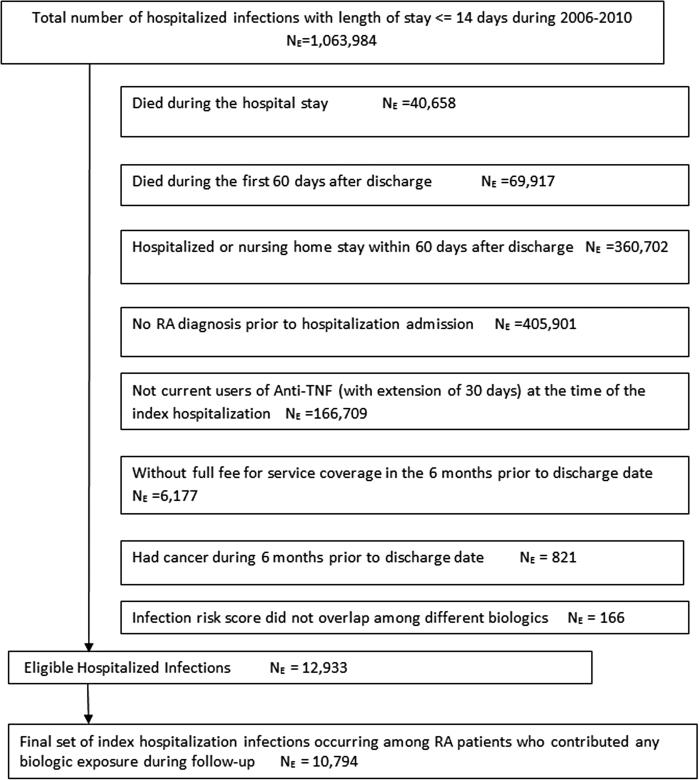
Using 2006-2010 Medicare data for 100% of beneficiaries with RA enrolled in Medicare, we identified patients hospitalised with an infection while on anti-TNF agents. Follow-up began 61 days after hospital discharge and ended at the earliest of: next infection, loss of Medicare coverage or 18 months after start of follow-up. We calculated the incidence rate of subsequent hospitalised infection for each biologic and used Cox regression to control for potential confounders.
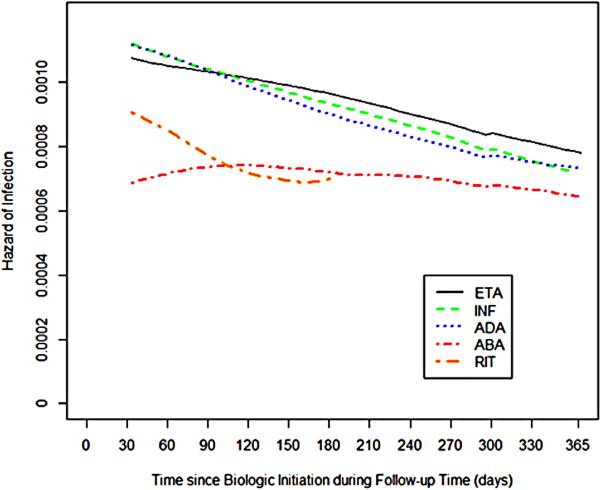
10 794 eligible hospitalised infections among 10183 unique RA patients who contributed at least 1 day of biologic exposure during follow-up. We identified 7807 person-years of exposure to selected biologics--333 abatacept, 133 rituximab and 7341 anti-TNFs (1797 etanercept, 1405 adalimumab, 4139 infliximab)--and 2666 associated infections. Mean age across biologic exposure cohorts was 64-69 years. The crude incidence rate of subsequent hospitalised infection ranged from 27.1 to 34.6 per 100 person-years. After multivariable adjustment, abatacept (HR: 0.80, 95% CI 0.64 to 0.99) and etanercept (HR: 0.83, 95% CI 0.72 to 0.96) users had significantly lower risks of subsequent infection compared to infliximab users.
Among RA patients who experienced a hospitalised infection while on anti-TNF therapy, abatacept and etanercept were associated with the lowest risk of subsequent infection compared to other biologic therapies.
类风湿关节炎(RA)患者在发生严重感染后接受生物治疗,其后续感染风险尚不清楚。
比较在接受抗肿瘤坏死因子(抗TNF)治疗期间曾因感染住院的RA患者中,与特定生物制剂相关的后续住院感染风险。
利用2006 - 2010年医疗保险中100%参保RA受益人的数据,我们确定了在使用抗TNF药物期间因感染住院的患者。随访在出院61天后开始,最早在以下情况结束:下次感染、失去医疗保险覆盖或随访开始后18个月。我们计算了每种生物制剂后续住院感染的发病率,并使用Cox回归来控制潜在的混杂因素。
在随访期间至少有1天生物制剂暴露的10183例独特RA患者中,有10794例符合条件的住院感染。我们确定了7807人年的选定生物制剂暴露时间——333人使用阿巴西普,133人使用利妥昔单抗,7341人使用抗TNF药物(1797人使用依那西普,1405人使用阿达木单抗,4139人使用英夫利昔单抗)——以及2666例相关感染。生物制剂暴露队列的平均年龄为64 - 69岁。后续住院感染的粗发病率为每100人年27.1至34.6例。多变量调整后,与使用英夫利昔单抗的患者相比,使用阿巴西普(HR:0.80,95%CI 0.64至0.99)和依那西普(HR:0.83,95%CI 0.72至0.96)的患者后续感染风险显著降低。
在接受抗TNF治疗期间发生过住院感染的RA患者中,与其他生物治疗相比,阿巴西普和依那西普的后续感染风险最低。