Ryan C J, Peng W, Kheoh T, Welkowsky E, Haqq C M, Chandler D W, Scher H I, Molina A
University of California San Francisco, San Francisco, CA, USA.
Janssen Research & Development, Los Angeles, CA, USA.
Prostate Cancer Prostatic Dis. 2014 Jun;17(2):192-8. doi: 10.1038/pcan.2014.8. Epub 2014 Mar 18.
We analyzed the potential of abiraterone acetate (henceforth abiraterone) to reduce androgen levels below lower limits of quantification (LLOQ) and explored the association with changes in PSA decline in metastatic castration-resistant prostate cancer (mCRPC) patients.
COU-AA-301 is a 2:1 randomized, double-blind, placebo-controlled study comparing abiraterone (1000 mg q.d.) plus low-dose prednisone (5 mg b.i.d.) with placebo plus prednisone in mCRPC patients post docetaxel. Serum testosterone, androstenedione and dehydroepiandrosterone sulfate from baseline to week 12 were measured by novel ultrasensitive two-dimensional liquid chromatography coupled to tandem mass spectrometry assays in a subset of subjects in each arm (abiraterone plus prednisone, n=80; prednisone, n=38). The association between PSA response (< or =50% baseline) and undetectable androgens (week 12 androgen level below LLOQ) was analyzed using logistic regression.
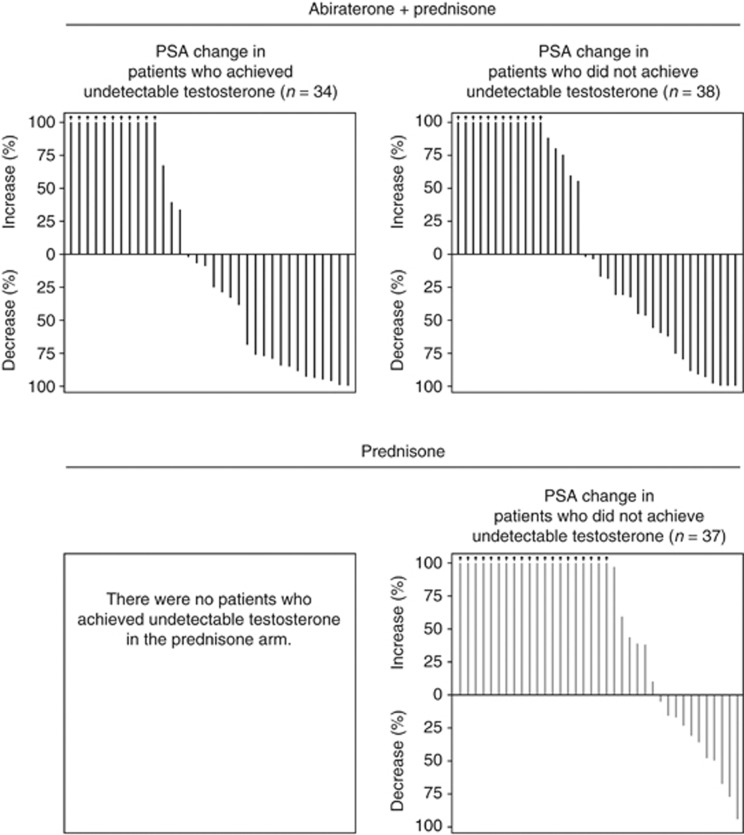
A significantly greater reduction in serum androgens was observed with abiraterone plus prednisone versus prednisone (all P < or = 0.0003), reaching undetectable levels for testosterone (47.2% versus 0%, respectively). A positive association was observed between achieving undetectable serum androgens and PSA decline (testosterone: odds ratio=1.54; 95% confidence interval: 0.546-4.347). Reduction of androgens to undetectable levels did not occur in all patients achieving a PSA response, and a PSA response did not occur in all patients achieving undetectable androgen levels.
Abiraterone plus prednisone significantly reduced serum androgens, as measured by ultrasensitive assays and was generally associated with PSA response. However, androgen decline did not uniformly predict PSA decline suggesting ligand-independent or other mechanisms for mCRPC progression.
我们分析了醋酸阿比特龙(以下简称阿比特龙)将雄激素水平降低至定量下限(LLOQ)以下的潜力,并探讨了其与转移性去势抵抗性前列腺癌(mCRPC)患者前列腺特异性抗原(PSA)下降变化之间的关联。
COU-AA-301是一项2:1随机、双盲、安慰剂对照研究,比较阿比特龙(1000毫克每日一次)联合低剂量泼尼松(5毫克每日两次)与安慰剂联合泼尼松用于多西他赛后的mCRPC患者。在每个治疗组的一部分受试者(阿比特龙联合泼尼松组,n = 80;泼尼松组,n = 38)中,采用新型超灵敏二维液相色谱-串联质谱分析法测量从基线到第12周的血清睾酮、雄烯二酮和硫酸脱氢表雄酮。使用逻辑回归分析PSA反应(≤50%基线)与不可检测的雄激素(第12周雄激素水平低于LLOQ)之间的关联。
与泼尼松相比,阿比特龙联合泼尼松治疗组血清雄激素水平显著降低(所有P≤0.0003),睾酮降至不可检测水平(分别为47.2%和0%)。血清雄激素不可检测与PSA下降之间存在正相关(睾酮:比值比 = 1.54;95%置信区间:0.546 - 4.347)。并非所有PSA反应的患者雄激素都降至不可检测水平,也并非所有雄激素水平不可检测的患者都出现PSA反应。
通过超灵敏检测法测定,阿比特龙联合泼尼松可显著降低血清雄激素水平,且通常与PSA反应相关。然而,雄激素下降并不能一致地预测PSA下降,提示mCRPC进展存在非配体依赖性或其他机制。