Bindoria Suchitra V, Devkar Ramesh, Gupta Indrani, Ranebennur Virupax, Saggurti Niranjan, Ramesh Sowmya, Deshmukh Dilip, Gaikwad Sanjeevsingh
FHI 360, Bandra (East), Mumbai 400051, India.
BMC Res Notes. 2014 Mar 26;7:177. doi: 10.1186/1756-0500-7-177.
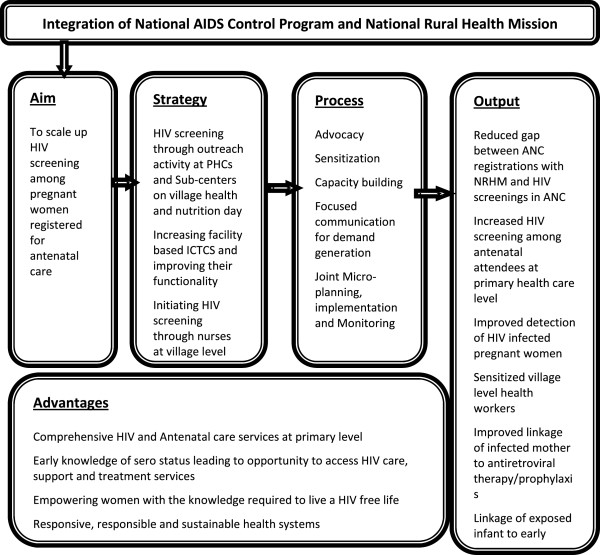
The objectives of this paper are: (1) to study the feasibility and relative benefits of integrating the prevention of parent-to-child transmission (PPTCT) component of the National AIDS Control Program with the maternal and child health component of the National Rural Health Mission (NRHM) by offering HIV screening at the primary healthcare level; and (2) to estimate the incremental cost-effectiveness ratio to understand whether the costs are commensurate with the benefits.
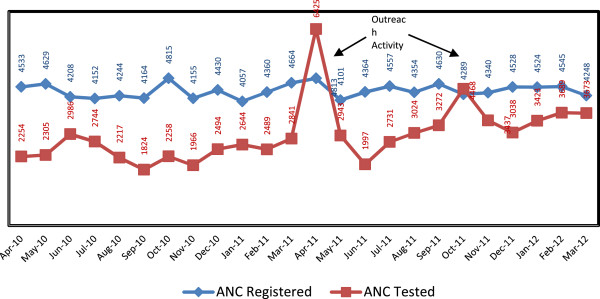
The intervention included advocacy with political, administrative/health heads, and capacity building of health staff in Satara district, Maharashtra, India. The intervention also conducted biannual outreach activities at primary health centers (PHCs)/sub-centers (SCs); initiated facility-based integrated counseling and testing centers (FICTCs) at all round-the-clock PHCs; made the existing FICTCs functional and trained PHC nurses in HIV screening. All "functional" FICTCs were equipped to screen for HIV and trained staff provided counseling and conducted HIV testing as per the national protocol. Data were collected pre- and post- integration on the number of pregnant women screened for HIV, the number of functional FICTCs and intervention costs. Trend analyses on various outcome measures were conducted. Further, the incremental cost-effectiveness ratio per pregnant woman screened was calculated.
An additional 27% of HIV-infected women were detected during the intervention period as the annual HIV screening increased from pre- to post-intervention (55% to 79%, p < 0.001) among antenatal care (ANC) attendees under the NRHM. A greater increase in HIV screening was observed in PHCs/SCs. The proportions of functional FICTCs increased from 47% to 97% (p < 0.001). Additionally, 93% of HIV-infected pregnant women were linked to anti-retroviral therapy centers; 92% of mother-baby pairs received Nevirapine; and 89% of exposed babies were enrolled for early infant diagnosis. The incremental cost-effectiveness ratio was estimated at INR 44 (less than 1 US$) per pregnant woman tested.
Integrating HIV screening with the broader Rural Health Mission is a promising opportunity to scale up the PPTCT program. However, advocacy, sensitization, capacity building and the judicious utilization of available resources are key to widening the reach of the PPTCT program in India and elsewhere.
本文的目标是:(1)通过在初级卫生保健层面提供艾滋病毒筛查,研究将国家艾滋病控制项目的预防母婴传播(PPTCT)部分与国家农村卫生使命(NRHM)的母婴健康部分相结合的可行性和相对益处;(2)估计增量成本效益比,以了解成本是否与效益相称。
干预措施包括与政治、行政/卫生部门负责人进行宣传,并对印度马哈拉施特拉邦萨塔拉区的卫生工作人员进行能力建设。干预措施还在初级卫生中心(PHCs)/分中心(SCs)每半年开展一次外展活动;在所有全天候的初级卫生中心设立基于机构的综合咨询和检测中心(FICTCs);使现有的FICTCs发挥作用,并对初级卫生中心的护士进行艾滋病毒筛查培训。所有“功能性”FICTCs都具备艾滋病毒筛查能力,训练有素的工作人员按照国家方案提供咨询并进行艾滋病毒检测。在整合前后收集了关于接受艾滋病毒筛查的孕妇数量、功能性FICTCs的数量和干预成本的数据。对各种结果指标进行了趋势分析。此外,计算了每名接受筛查的孕妇的增量成本效益比。
在干预期间,检测出另外27%的艾滋病毒感染妇女,因为在国家农村卫生使命下的产前护理(ANC)就诊者中,艾滋病毒年度筛查从干预前到干预后有所增加(从55%增至79%,p<0.001)。在初级卫生中心/分中心观察到艾滋病毒筛查有更大幅度的增加。功能性FICTCs的比例从47%增至97%(p<0.001)。此外,93%的艾滋病毒感染孕妇被转介到抗逆转录病毒治疗中心;92%的母婴对接受了奈韦拉平治疗;89%的受感染婴儿登记接受早期婴儿诊断。估计每名接受检测的孕妇的增量成本效益比为44印度卢比(不到1美元)。
将艾滋病毒筛查与更广泛的农村卫生使命相结合是扩大预防母婴传播项目规模的一个有前景的机会。然而,宣传、提高认识、能力建设和明智利用现有资源是在印度和其他地方扩大预防母婴传播项目覆盖范围的关键。