Aihara Hiroyuki, Kumar Nitin, Ryou Marvin, Abidi Wasif, Ryan Michele B, Thompson Christopher C
Developmental Endoscopy, Division of Gastroenterology, Hepatology and Endoscopy, Brigham and Women's Hospital, Boston, Massachusetts, USA.
Gastrointest Endosc. 2014 Sep;80(3):495-502. doi: 10.1016/j.gie.2014.01.050. Epub 2014 Mar 27.
The lack of countertraction in endoscopic submucosal dissection (ESD) results in increased technical demand and procedure time. Although the suture-pulley method for countertraction has been reported, its effectiveness compared with the traditional ESD technique remains unclear.
To objectively analyze efficacy of countertraction using the suture-pulley method for ESD.
Prospective ex vivo animal study.
Animal laboratory.
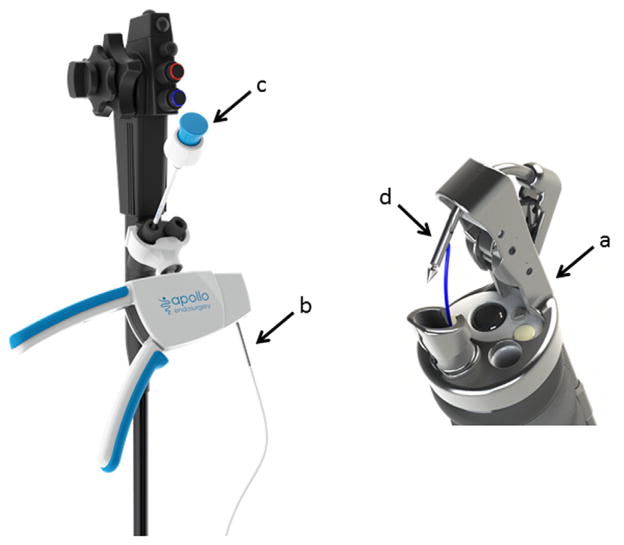
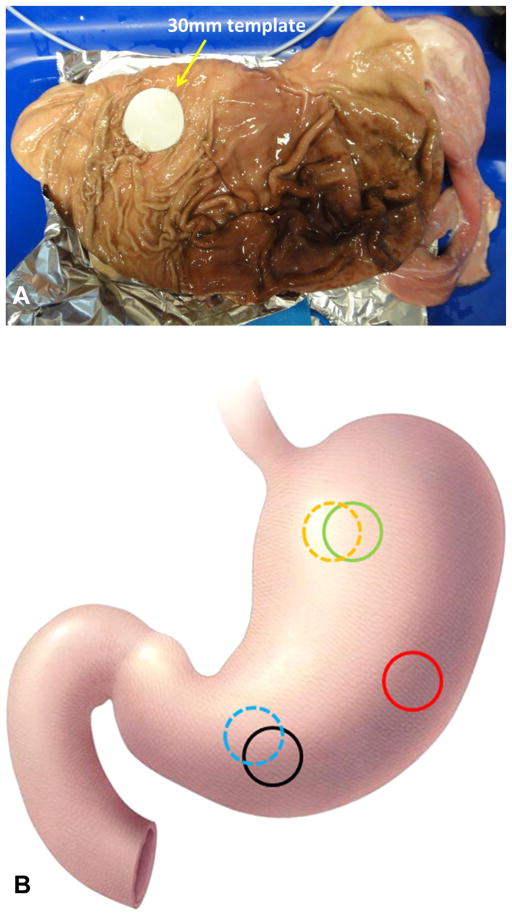
Twenty simulated gastric lesions were created in porcine stomachs by using a standard circular template 30 mm in diameter. In the control arm (n = 10), ESD was performed by using the standard technique. In the suture-pulley arm (N = 10), a circumferential incision was made, and an endoscopic suturing device was used to place the suture pulley.
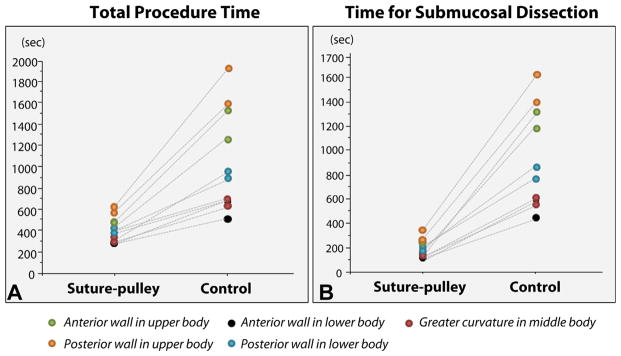
The primary outcome of this study was total procedure time.
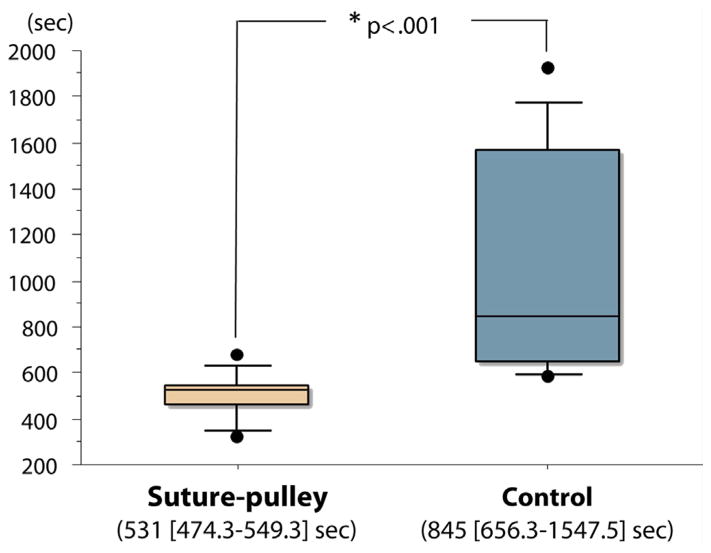
The median total procedure time with the suture-pulley method was significantly shorter than the traditional ESD technique (median, 25% to 75%, interquartile range [IQR]: 531 seconds [474.3-549.3 seconds] vs 845 seconds [656.3-1547.5 seconds], P < .001). The median time (IQR) for suture-pulley placement was 160.5 seconds (150.0-168.8 seconds). Although there was a significantly longer procedure time for proximal versus middle/lower stomach lesions with traditional ESD (median, 1601 seconds; IQR, 1547.5-1708.8 seconds vs median, 663 seconds; IQR, 627.5-681.8 seconds; P = .01), there was no significant difference in procedure time for lesions of various locations when using the suture-pulley method. Compared with traditional ESD, the suture-pulley method was less demanding in all categories evaluated by the NASA Task Load Index.
Ex vivo study.
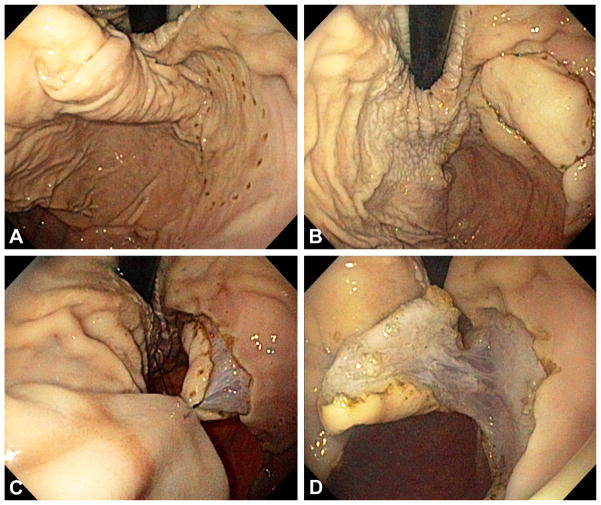
The suture-pulley method facilitates direct visualization of the submucosal layer during ESD and significantly reduces procedure time and technical difficulty. In addition, the benefit of the suture-pulley method was seen for both simple and more complicated ESDs.
内镜黏膜下剥离术(ESD)中缺乏对抗牵引会导致技术要求提高和手术时间延长。尽管已报道了用于对抗牵引的缝合滑轮法,但其与传统ESD技术相比的有效性仍不明确。
客观分析使用缝合滑轮法进行ESD对抗牵引的疗效。
前瞻性体外动物研究。
动物实验室。
使用直径30mm的标准圆形模板在猪胃中制造20个模拟胃病变。在对照组(n = 10)中,采用标准技术进行ESD。在缝合滑轮组(n = 10)中,进行环形切口,并使用内镜缝合装置放置缝合滑轮。
本研究的主要结果是总手术时间。
缝合滑轮法的中位总手术时间明显短于传统ESD技术(中位数,25%至75%,四分位间距[IQR]:531秒[474.3 - 549.3秒]对845秒[656.3 - 1547.5秒],P <.001)。放置缝合滑轮的中位时间(IQR)为160.5秒(150.0 - 168.8秒)。尽管传统ESD治疗胃近端病变的手术时间明显长于胃中/下部病变(中位数,1601秒;IQR,1547.5 - 1708.8秒对中位数,663秒;IQR,627.5 - 681.8秒;P =.01),但使用缝合滑轮法时不同部位病变的手术时间无显著差异。与传统ESD相比,在NASA任务负荷指数评估的所有类别中,缝合滑轮法的要求更低。
体外研究。
缝合滑轮法有助于在ESD期间直接观察黏膜下层,并显著减少手术时间和技术难度。此外,简单和复杂的ESD均可见到缝合滑轮法的益处。