Tran Hanh, Turingan Isidro, Zajkowska Marta, Tran Kim
Discipline of Surgery, Sydney Medical School, University of Sydney, Westmead Hospital, Westmead, NSW, Australia; The Sydney Hernia Specialists Clinic, Level 2, 195 Macquarie St, Sydney NSW 2000, Australia.
The Sydney Hernia Specialists Clinic, Sydney, NSW, Australia.
JSLS. 2014 Jan-Mar;18(1):34-40. doi: 10.4293/108680813X13693422519190.
Laparoscopic parastomal hernia repair with modified Sugarbaker technique has become increasingly the operation of choice because of its low recurrence rates. This study aimed to assess feasibility, safety, and efficiency of performing the same operation with single-incision laparoscopic surgery.
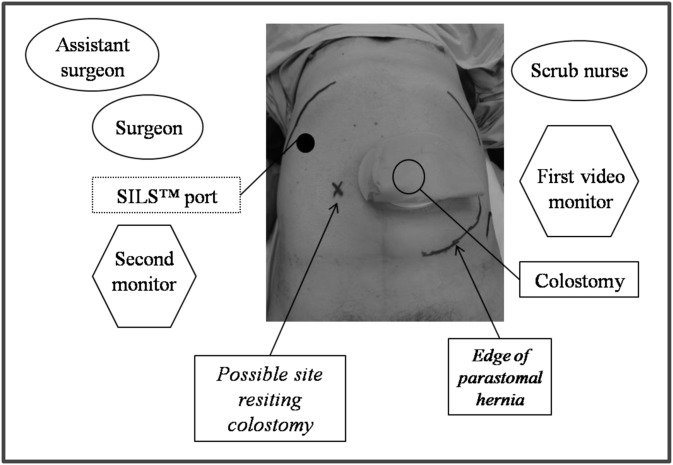
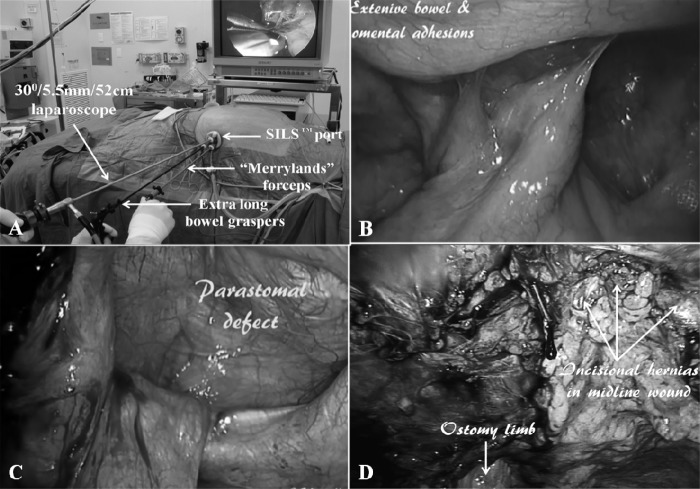
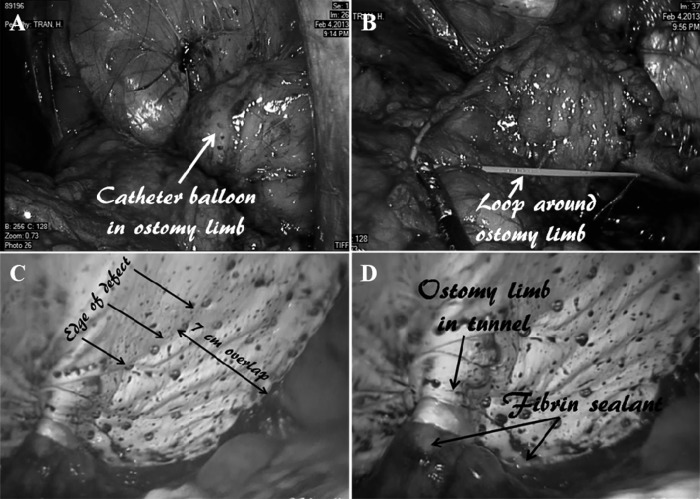
All patients referred from March 2010 to February 2013 were considered for single-port laparoscopic repair with modified Sugarbaker technique. A SILS port (Covidien, Norwalk, Connecticut, USA) was used together with conventional straight dissecting instruments and a 5.5- mm/52-cm/30° laparoscope. Important technical aspects include modified dissection techniques, namely, "inline" and "chopsticks" to overcome loss of triangulation, insertion of a urinary catheter into an ostomy for ostomy limb identification, safe adhesiolysis by avoiding electocautery, saline -jet dissection to demarcate tissue planes, dissection of an entire laparotomy scar to expose incidental incisional hernias, adequate mobilization of an ostomy limb for lateralization, and wide overlapping of defect with antiadhesive mesh.
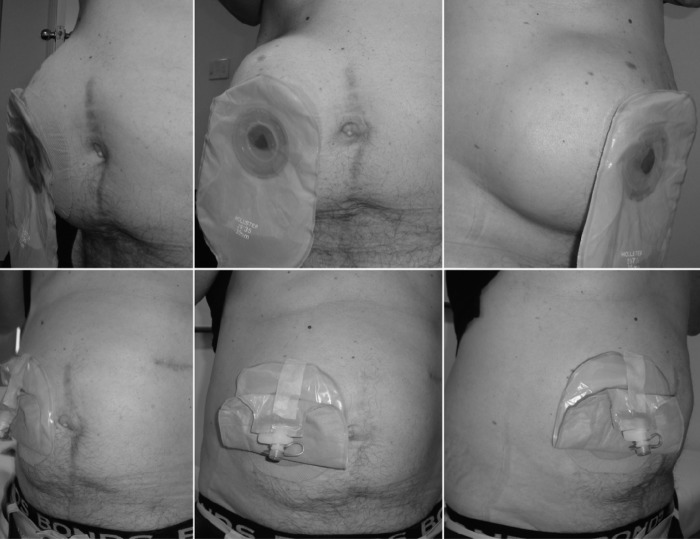
Of 6 patients, 5 underwent single-port laparoscopic repair, and 1 (whose body mass index [BMI] of 39.4 kg/m(2) did not permit SILS port placement) underwent multiport repair. Mean defect size was 10 cm, and mean mesh size was 660 cm(2) with 4 patients having incidental incisional hernias repaired by the same mesh. Mean operation time was 270 minutes, and mean hospital stay was 4 days. Appliance malfunction ceased immediately, and pain associated with parastomal hernia disappeared. There was no recurrence with a follow-up of 2 to 36 months.
Compared with multiport repair, single-port laparoscopic parastomal repair with modified Sugarbaker technique is safe and efficient, and it may eventually become the standard of care.
改良Sugarbaker技术的腹腔镜造口旁疝修补术因其低复发率日益成为首选术式。本研究旨在评估单切口腹腔镜手术实施该术式的可行性、安全性及有效性。
2010年3月至2013年2月收治的所有患者均考虑采用改良Sugarbaker技术行单孔腹腔镜修补术。使用一个SILS端口(美国康涅狄格州诺沃克市柯惠医疗公司生产),同时使用传统的直式解剖器械及一台5.5毫米/52厘米/30°的腹腔镜。重要的技术要点包括改良的解剖技术,即“直线式”和“筷子式”以克服三角定位的缺失,将导尿管插入造口以识别造口肠管,通过避免电灼进行安全的粘连松解,用生理盐水喷射解剖来界定组织层面,解剖整个剖腹手术瘢痕以暴露偶然发现的切口疝,充分游离造口肠管以便向外侧移位,以及用抗粘连补片广泛重叠覆盖缺损。
6例患者中,5例行单孔腹腔镜修补术,1例(体重指数[BMI]为39.4kg/m²,不适合放置SILS端口)行多孔修补术。平均缺损大小为10厘米,平均补片大小为660平方厘米,4例偶然发现的切口疝患者用同一补片修补。平均手术时间为270分钟,平均住院时间为4天。器械故障立即停止,造口旁疝相关疼痛消失。随访2至36个月无复发。
与多孔修补术相比,改良Sugarbaker技术的单孔腹腔镜造口旁修补术安全有效,最终可能成为标准术式。