Clinic for Oncology, Hematology, and Palliative Medicine, Marien Hospital Dusseldorf, Dusseldorf, Germany.
Cancer. 2014 Jun 15;120(12):1838-46. doi: 10.1002/cncr.28663. Epub 2014 Apr 4.
Thrombocytopenia in patients with myelodysplastic syndrome (MDS) is associated with shortened survival and an increased risk of evolution to acute myeloid leukemia (AML). In this study, the authors evaluated the efficacy of romiplostim in patients who had thrombocytopenia with low-risk/intermediate-1-risk MDS.
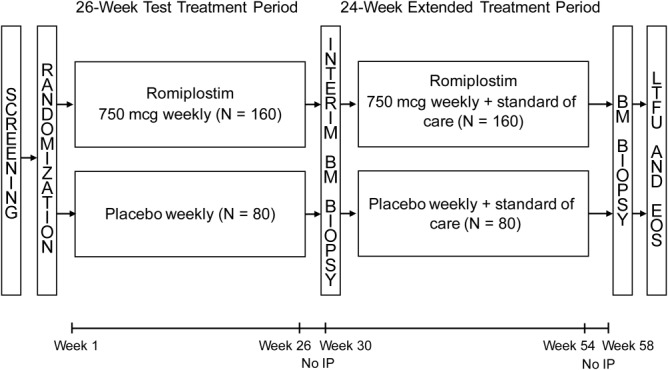
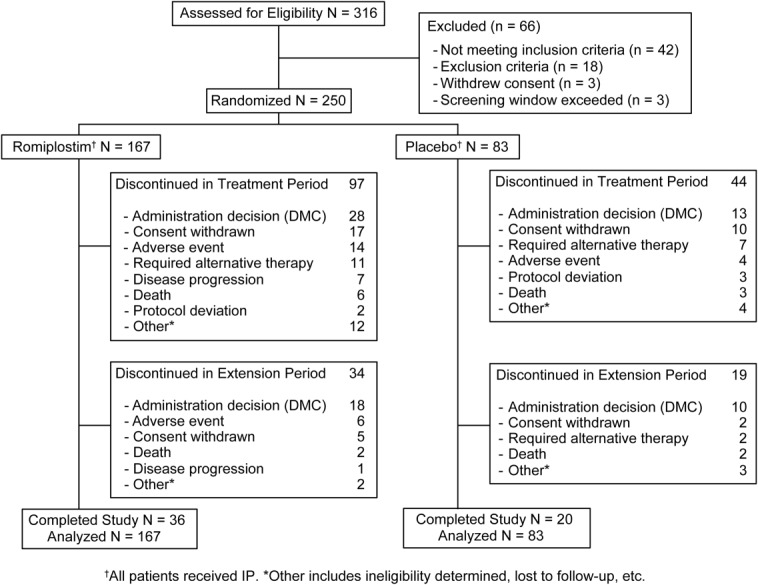
Patients who had thrombocytopenia with low-risk/intermediate-1-risk MDS (N = 250) were randomized 2:1 to receive romiplostim or placebo weekly for 58 weeks.
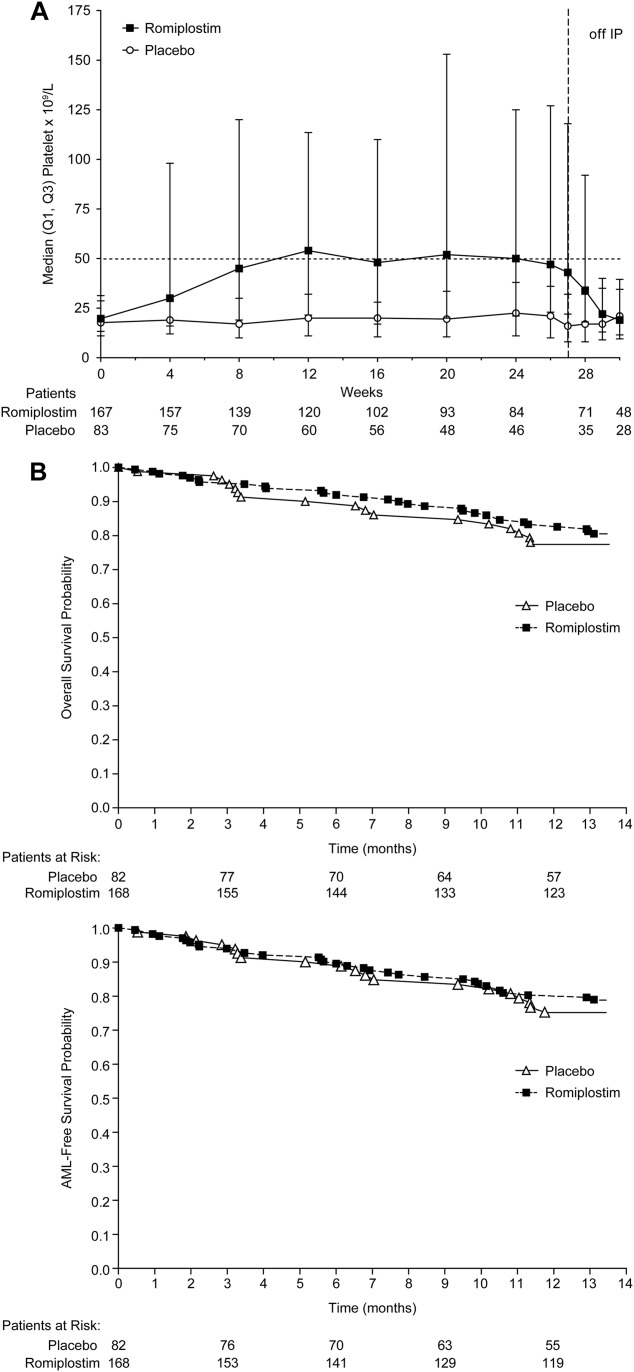
The primary endpoint- the number of clinically significant bleeding events (CSBEs) per patient-had a hazard ratio for romiplostim:placebo of 0.83 (95% confidence interval, 0.66-1.05; P = .13). CSBEs were reduced significantly in the romiplostim group for patients who had baseline platelet counts ≥20 × 10(9) /L (P < .0001). For patients who had baseline platelet counts <20 × 10(9) /L, there was no difference in the number of CSBEs, but the platelet transfusion rates were higher in the placebo group (P < .0001), which may have affected the overall CSBE results in this group with severe thrombocytopenia. The incidence of bleeding events was reduced significantly in the romiplostim group (relative risk, 0.92), as were protocol-defined platelet transfusions (relative risk, 0.77). Platelet response rates according to 2006 International Working Group criteria were higher for the group that received romiplostim (odds ratio, 15.6). On the basis of interim data, an independent data monitoring committee advised halting study drug because of concerns regarding excess blasts and AML rates with romiplostim (interim hazard ratio, 2.51). At 58 weeks, the AML rates were 6% in the romiplostim group and 4.9% in the placebo group (hazard ratio, 1.20; 95% confidence interval, 0.38-3.84), and the overall survival rates were similar.
Romiplostim treatment in patients with low-risk/intermediate-1-risk MDS increased platelet counts and decreased the number of bleeding events and platelet transfusions. Although study drug was discontinued because of an initial concern of AML risk, survival and AML rates were similar with romiplostim and placebo.
骨髓增生异常综合征(MDS)患者的血小板减少与生存期缩短和向急性髓系白血病(AML)演变的风险增加有关。在这项研究中,作者评估了罗米司亭在低危/中危-1 风险 MDS 伴血小板减少症患者中的疗效。
250 名低危/中危-1 风险 MDS 伴血小板减少症患者被随机分为 2:1 组,分别接受每周罗米司亭或安慰剂治疗 58 周。
主要终点——每位患者的临床显著出血事件(CSBE)数量——罗米司亭的风险比为安慰剂的 0.83(95%置信区间,0.66-1.05;P=0.13)。对于基线血小板计数≥20×10(9)/L 的患者,罗米司亭组的 CSBE 显著减少(P<0.0001)。对于基线血小板计数<20×10(9)/L 的患者,CSBE 数量没有差异,但安慰剂组的血小板输注率更高(P<0.0001),这可能影响了该组严重血小板减少症患者的总体 CSBE 结果。罗米司亭组的出血事件发生率显著降低(相对风险,0.92),根据方案定义的血小板输注也显著降低(相对风险,0.77)。根据 2006 年国际工作组标准,接受罗米司亭治疗的患者血小板反应率更高(优势比,15.6)。基于中期数据,一个独立的数据监测委员会建议因罗米司亭的过度原始细胞和 AML 发生率而停止研究药物(中期风险比,2.51)。在 58 周时,罗米司亭组的 AML 发生率为 6%,安慰剂组为 4.9%(风险比,1.20;95%置信区间,0.38-3.84),总体生存率相似。
罗米司亭治疗低危/中危-1 风险 MDS 患者可增加血小板计数,并减少出血事件和血小板输注的数量。尽管因最初对 AML 风险的担忧而停用研究药物,但罗米司亭与安慰剂的生存率和 AML 发生率相似。