Dingemans Anne-Marie C, Bootsma Gerben, van Baardwijk Angela, Reymen Bart, Wanders Rinus, Brans Boudewijn, Das Marco, Hochstenbag Monique, van Belle Arne, Houben Ruud, Lambin Philippe, de Ruysscher Dirk
*Department of Pulmonology, GROW School for Oncology and Developmental Biology, Maastricht University Medical Centre, Maastricht, The Netherlands; †Department of Pulmonology, Atrium Medical Centre, Heerlen, The Netherlands; ‡Department of Radiation Oncology (MAASTRO Clinic), GROW School for Oncology and Developmental Biology; §Department of Nuclear Medicine, and ‖Department of Radiology, GROW School for Oncology and Developmental Biology, Maastricht University Medical Centre, Maastricht, The Netherlands; and ¶Department of Radiation Oncology, University Hospitals Leuven/KU Leuven, Leuven, Belgium.
J Thorac Oncol. 2014 May;9(5):710-6. doi: 10.1097/JTO.0000000000000151.
In this open-label phase I study, the maximum-tolerated dose of cetuximab with concurrent chemoradiotherapy (C-CRT) in stage III non-small-cell lung cancer together with individualized, isotoxic accelerated radiotherapy (RT) was investigated.
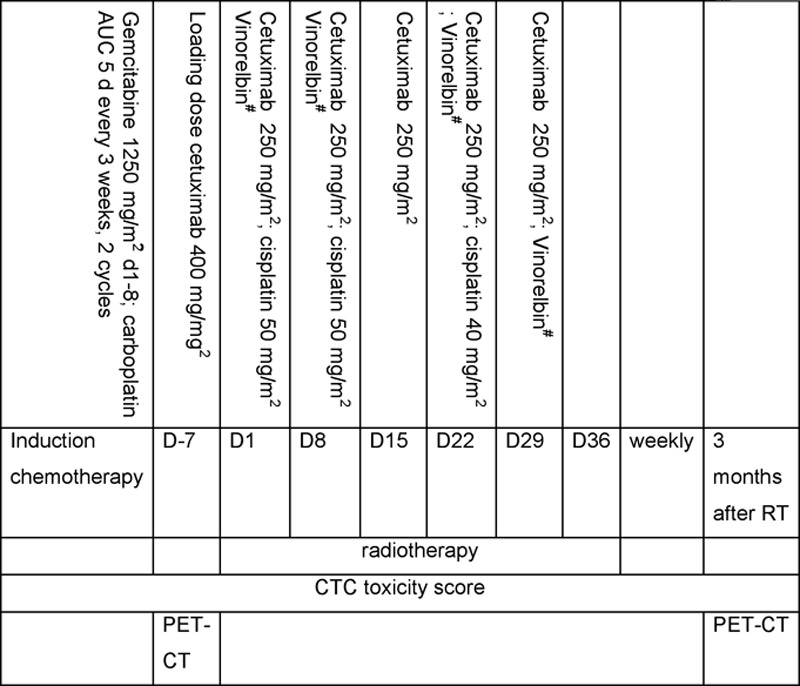
Patients with stage III non-small-cell lung cancer, World Health Organization performance status 0-1, forced expiratory volume in 1 second more than 50%, carbon monoxide diffusing capacity more than 50%, weight loss less than 10%, and no severe comorbidity were enrolled. Patients without progression after one to two cycles of gemcitabine-carboplatin were included and treated with cetuximab 400 mg/kg d7 and 250 mg/kg weekly together with RT and cisplatin (50 mg/m d1, 8; 40 mg/m d22)-vinorelbine for 5 weeks. Vinorelbine was escalated in three steps; (1) 10 mg/m d1, 8 and 8 mg/m d22, 29; (2) 20 mg/m d1, 8 and 8 mg/m d22, 29; (3) 20 mg/m d1, 8; 15 mg/m d22, 29. An individualized prescribed RT dose based on normal tissue dose constraints was applied (e.g., mean lung dose 19 Gy). The primary endpoint was the maximum-tolerated dose 3 months after the end of C-CRT; secondary endpoints were toxicity and metabolic response as assessed by positron emission tomography.
Between September 2007 and October 2010, 25 patients (12 men, 13 women, mean age 59 years) were included. The mean RT dose was 62 ± 6.6 Gy. The vinorelbine dose could be escalated to dose level 3. Twelve of 25 patients experienced greater than or equal to grade 3 toxicity (esophagitis 3, rash 1, diarrhea 1, cough 1, dyspnea 1, vomiting 1, and pulmonary embolism 1). No dose-limiting toxicities were observed. One patient with a complete pathological response in dose level 3 developed a fatal hemoptysis 4 months after RT. Metabolic remissions were observed in 19 of 22 patients.
C-CRT with cetuximab and cisplatin-vinorelbine is safe to deliver at full dose. The recommended phase II dose is therefore cetuximab 400 mg/m d7 and 250 mg/m weekly, cisplatin 50 mg/m d1, 8; 40 mg/m d22 and vinorelbine 20 mg/m d1, 8; 15 mg/m d22, 29 for 5 weeks together with RT.
在这项开放标签的I期研究中,研究了西妥昔单抗与同步放化疗(C-CRT)联合用于III期非小细胞肺癌时的最大耐受剂量,同时采用个体化、等毒性加速放疗(RT)。
纳入III期非小细胞肺癌患者,世界卫生组织体能状态为0 - 1,1秒用力呼气量超过50%,一氧化碳弥散能力超过50%,体重减轻少于10%,且无严重合并症。在接受一至两个周期吉西他滨 - 卡铂治疗后无进展的患者被纳入,给予西妥昔单抗400 mg/kg第7天和250 mg/kg每周一次,同时联合放疗和顺铂(50 mg/m²第1、8天;40 mg/m²第22天)-长春瑞滨治疗5周。长春瑞滨分三步递增;(1)10 mg/m²第1、8天和8 mg/m²第22、29天;(2)20 mg/m²第1、8天和8 mg/m²第22、29天;(3)20 mg/m²第1、8天;15 mg/m²第22、29天。根据正常组织剂量限制应用个体化规定的放疗剂量(例如,平均肺剂量19 Gy)。主要终点是C-CRT结束后3个月的最大耐受剂量;次要终点是毒性和通过正电子发射断层扫描评估的代谢反应。
2007年9月至2010年10月,纳入25例患者(12例男性,13例女性,平均年龄59岁)。平均放疗剂量为62 ± 6.6 Gy。长春瑞滨剂量可递增至剂量水平3。25例患者中有12例经历了≥3级毒性(食管炎3例、皮疹1例、腹泻1例、咳嗽1例、呼吸困难1例、呕吐1例、肺栓塞1例)。未观察到剂量限制性毒性。1例在剂量水平3出现完全病理缓解的患者在放疗后4个月发生致命性咯血。22例患者中有19例观察到代谢缓解。
西妥昔单抗与顺铂 - 长春瑞滨联合C-CRT全剂量给药是安全的。因此,推荐的II期剂量为西妥昔单抗400 mg/m²第7天和250 mg/m²每周一次,顺铂50 mg/m²第1、8天;40 mg/m²第22天以及长春瑞滨20 mg/m²第1、8天;15 mg/m²第22、29天,联合放疗共5周。