Müller-Redetzky Holger C, Will Daniel, Hellwig Katharina, Kummer Wolfgang, Tschernig Thomas, Pfeil Uwe, Paddenberg Renate, Menger Michael D, Kershaw Olivia, Gruber Achim D, Weissmann Norbert, Hippenstiel Stefan, Suttorp Norbert, Witzenrath Martin
Crit Care. 2014 Apr 14;18(2):R73. doi: 10.1186/cc13830.
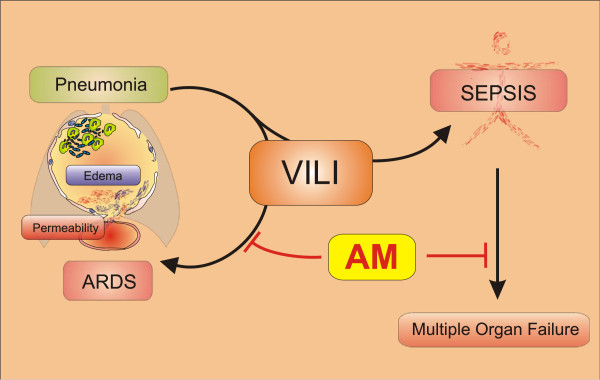
Ventilator-induced lung injury (VILI) contributes to morbidity and mortality in acute respiratory distress syndrome (ARDS). Particularly pre-injured lungs are susceptible to VILI despite protective ventilation. In a previous study, the endogenous peptide adrenomedullin (AM) protected murine lungs from VILI. We hypothesized that mechanical ventilation (MV) contributes to lung injury and sepsis in pneumonia, and that AM may reduce lung injury and multiple organ failure in ventilated mice with pneumococcal pneumonia.
We analyzed in mice the impact of MV in established pneumonia on lung injury, inflammation, bacterial burden, hemodynamics and extrapulmonary organ injury, and assessed the therapeutic potential of AM by starting treatment at intubation.
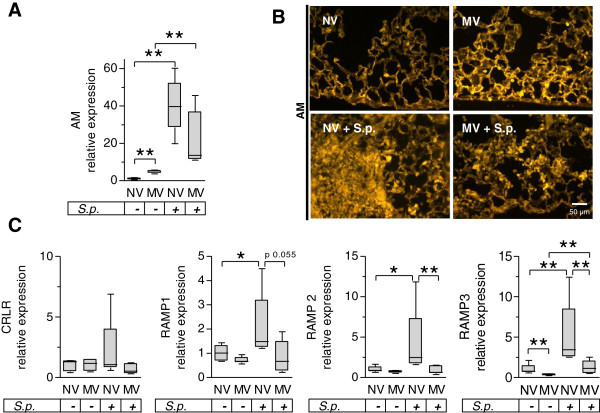
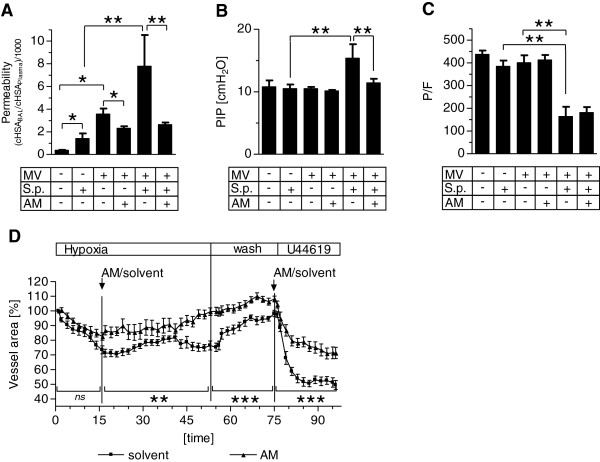
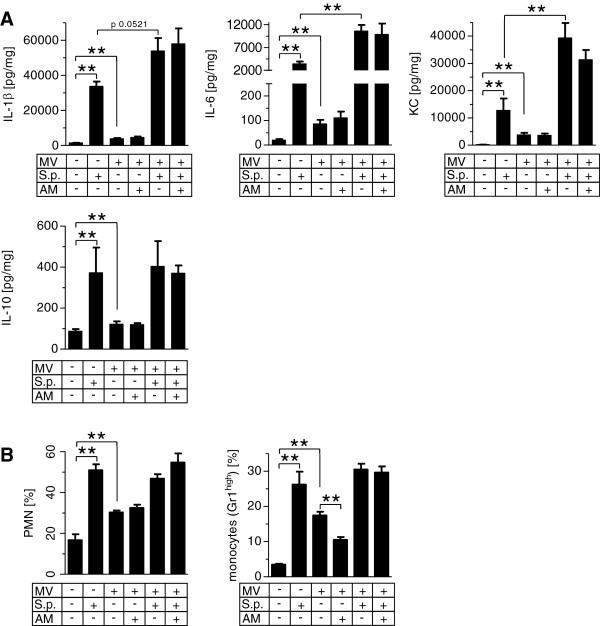
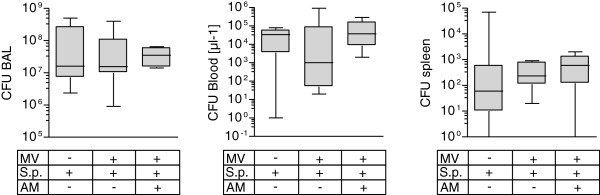
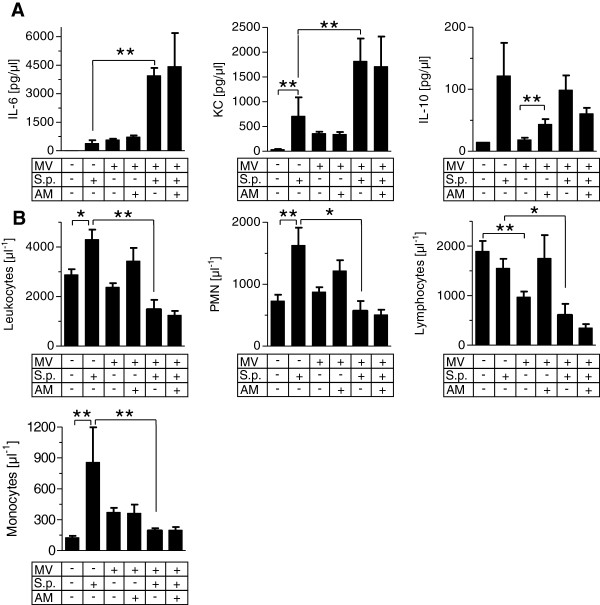
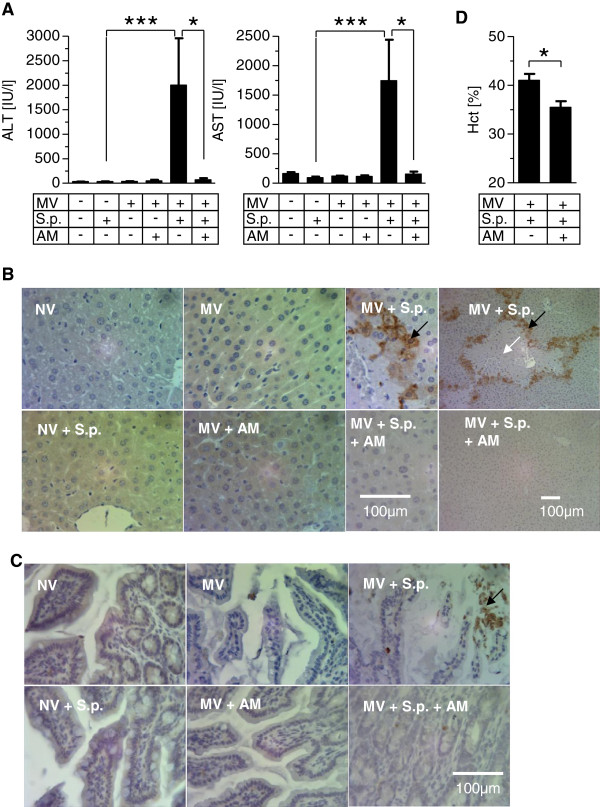
In pneumococcal pneumonia, MV increased lung permeability, and worsened lung mechanics and oxygenation failure. MV dramatically increased lung and blood cytokines but not lung leukocyte counts in pneumonia. MV induced systemic leukocytopenia and liver, gut and kidney injury in mice with pneumonia. Lung and blood bacterial burden was not affected by MV pneumonia and MV increased lung AM expression, whereas receptor activity modifying protein (RAMP) 1-3 expression was increased in pneumonia and reduced by MV. Infusion of AM protected against MV-induced lung injury (66% reduction of pulmonary permeability p < 0.01; prevention of pulmonary restriction) and against VILI-induced liver and gut injury in pneumonia (91% reduction of AST levels p < 0.05, 96% reduction of alanine aminotransaminase (ALT) levels p < 0.05, abrogation of histopathological changes and parenchymal apoptosis in liver and gut).
MV paved the way for the progression of pneumonia towards ARDS and sepsis by aggravating lung injury and systemic hyperinflammation leading to liver, kidney and gut injury. AM may be a promising therapeutic option to protect against development of lung injury, sepsis and extrapulmonary organ injury in mechanically ventilated individuals with severe pneumonia.
呼吸机诱导的肺损伤(VILI)可导致急性呼吸窘迫综合征(ARDS)的发病和死亡。尽管采用了保护性通气策略,但尤其预先受损的肺对VILI仍很敏感。在先前的一项研究中,内源性肽肾上腺髓质素(AM)可保护小鼠肺免受VILI损伤。我们推测机械通气(MV)会导致肺炎患者发生肺损伤和脓毒症,且AM可能会减轻肺炎通气小鼠的肺损伤和多器官功能衰竭。
我们分析了在已确诊肺炎的小鼠中MV对肺损伤、炎症、细菌负荷、血流动力学和肺外器官损伤的影响,并通过在插管时开始治疗来评估AM的治疗潜力。
在肺炎球菌肺炎中,MV增加了肺通透性,使肺力学和氧合功能衰竭恶化。MV显著增加了肺炎小鼠肺和血液中的细胞因子,但未增加肺白细胞计数。MV导致肺炎小鼠出现全身性白细胞减少以及肝、肠和肾损伤。MV肺炎对肺和血液中的细菌负荷无影响,且MV增加了肺AM表达,而受体活性修饰蛋白(RAMP)1-3表达在肺炎时增加,在MV作用下降低。输注AM可预防MV诱导的肺损伤(肺通透性降低66%,p<0.01;预防肺限制性通气)以及肺炎中VILI诱导的肝和肠损伤(天冬氨酸转氨酶(AST)水平降低91%,p<0.05;丙氨酸转氨酶(ALT)水平降低96%,p<0.05;消除肝和肠的组织病理学变化及实质细胞凋亡)。
MV通过加重肺损伤和全身性炎症反应导致肝、肾和肠损伤,为肺炎向ARDS和脓毒症的进展铺平了道路。AM可能是一种有前景的治疗选择,可预防机械通气的重症肺炎患者发生肺损伤、脓毒症和肺外器官损伤。