Serana Federico, Imberti Luisa, Amato Maria Pia, Comi Giancarlo, Gasperini Claudio, Ghezzi Angelo, Martinelli Vittorio, Provinciali Leandro, Rottoli Maria Rosa, Sotgiu Stefano, Stecchi Sergio, Vecchio Michele, Zaffaroni Mauro, Cordioli Cinzia, Capra Ruggero
CREA, Diagnostics Department, Spedali Civili of Brescia, Brescia, Italy.
Department NEUROFARBA, Neuroscience Section, University of Florence, Florence, Italy.
PLoS One. 2014 Apr 14;9(4):e94794. doi: 10.1371/journal.pone.0094794. eCollection 2014.
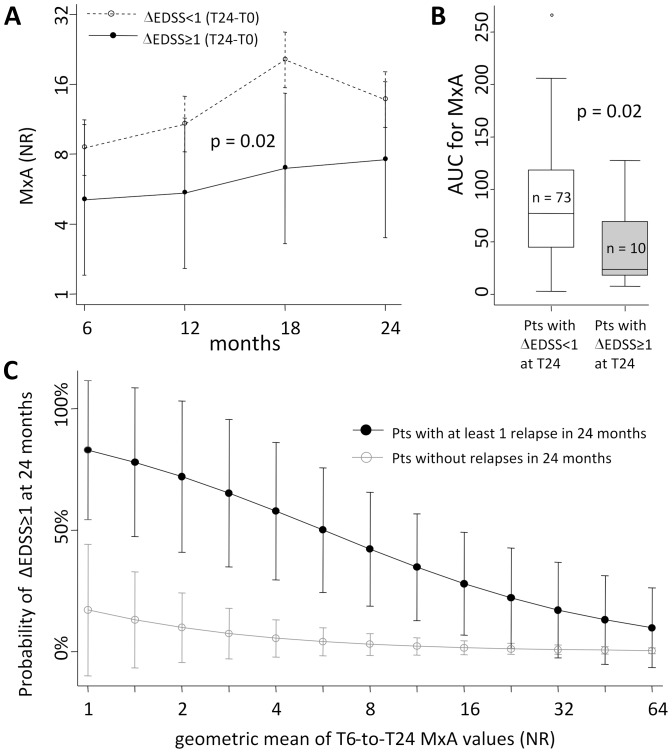
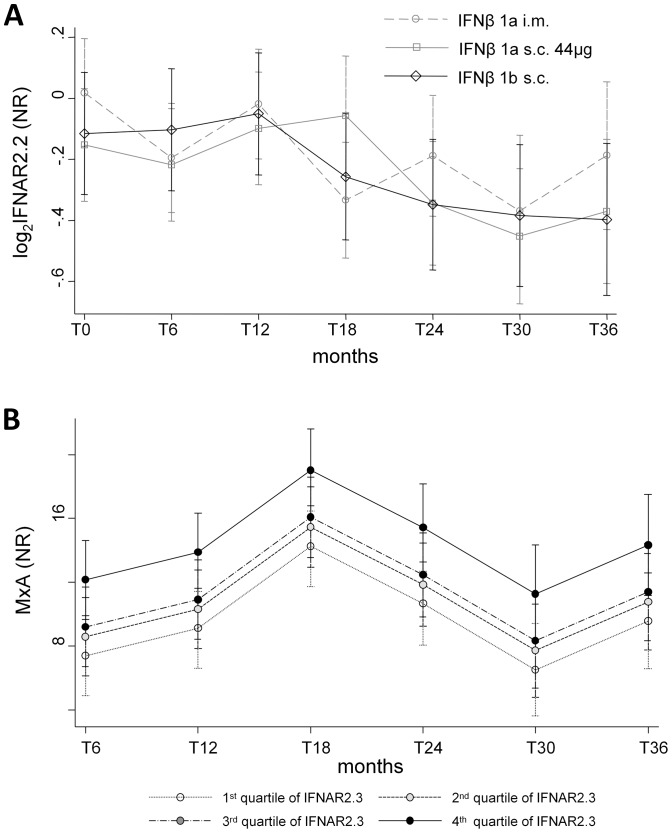
Even though anti-interferon beta (IFNβ) antibodies are the main determinants of IFNβ bioactivity loss and Myxovirus-resistance protein A (MxA) is the most established marker of IFNβ biological activity in IFNβ-treated multiple sclerosis patients, their usefulness in the routine clinical practice is still debated. Therefore, 118 multiple sclerosis patients naïve for treatment were enrolled for a 3-year longitudinal observational study mimicking the conditions of a real-world setting. In order to evaluate the kinetics of bioactivity loss in blood samples obtained every 6 months after therapy initiation, MxA and interferon receptor isoform/subunit mRNA were quantified by real-time PCR, anti-IFNβ binding antibodies were detected by radioimmunoprecipitation, and neutralizing antibodies by cytopathic effect inhibition assay. Clinical measures of disease activity and disability progression were also obtained at all time points. We found that, at the individual-patient level, the response to IFNβ therapy was extremely heterogeneous, including patients with stable or transitory, early or late loss of IFNβ bioactivity, and patients with samples lacking MxA mRNA induction in spite of absence of antibodies. No interferon receptor isoform alterations that could explain these findings were found. At the group level, none of these biological features correlated with the measures of clinical disease activity or progression. However, when MxA mRNA was evaluated not at the single time point as a dichotomic marker (induced vs. non-induced), but as the mean of its values measured over the 6-to-24 month period, the increasing average MxA predicted a decreasing risk of short-term disability progression, independently from the presence of relapses. Therefore, a more bioactive treatment, even if unable to suppress relapses, reduces their severity by an amount that is proportional to MxA levels. Together with its feasibility in the routine laboratory setting, these data warrant the quantification of MxA mRNA as a primary tool for a routine monitoring of IFNβ therapy.
尽管抗干扰素β(IFNβ)抗体是IFNβ生物活性丧失的主要决定因素,且黏液病毒抗性蛋白A(MxA)是IFNβ治疗的多发性硬化症患者中IFNβ生物活性最确定的标志物,但它们在常规临床实践中的实用性仍存在争议。因此,118例未经治疗的多发性硬化症患者被纳入一项为期3年的纵向观察性研究,该研究模拟了真实世界的情况。为了评估治疗开始后每6个月采集的血液样本中生物活性丧失的动力学,通过实时PCR对MxA和干扰素受体异构体/亚基mRNA进行定量,通过放射免疫沉淀检测抗IFNβ结合抗体,并通过细胞病变效应抑制试验检测中和抗体。在所有时间点还获得了疾病活动和残疾进展的临床指标。我们发现,在个体患者水平上,对IFNβ治疗的反应极其异质,包括IFNβ生物活性稳定或短暂、早期或晚期丧失的患者,以及尽管没有抗体但样本中缺乏MxA mRNA诱导的患者。未发现可解释这些发现的干扰素受体异构体改变。在组水平上,这些生物学特征均与临床疾病活动或进展指标无关。然而,当不是将MxA mRNA作为二分标志物(诱导与未诱导)在单个时间点进行评估,而是将其在6至24个月期间测量的值的平均值进行评估时,平均MxA增加预示着短期残疾进展风险降低,与复发的存在无关。因此,一种生物活性更高的治疗方法,即使无法抑制复发,也会按与MxA水平成比例的量降低其严重程度。连同其在常规实验室环境中的可行性,这些数据证明将MxA mRNA定量作为IFNβ治疗常规监测的主要工具是合理的。