Lucas Aimee L, Frado Laura E, Hwang Caroline, Kumar Sheila, Khanna Lauren G, Levinson Elana J, Chabot John A, Chung Wendy K, Frucht Harold
Division of Gastroenterology, Icahn School of Medicine at Mount Sinai, New York, New York.
Cancer. 2014 Jul 1;120(13):1960-7. doi: 10.1002/cncr.28662. Epub 2014 Apr 15.
Approximately 10% of pancreatic ductal adenocarcinoma (PDAC) is due to a genetic predisposition, including the breast and ovarian cancer syndrome germline mutations BRCA1 and BRCA2. Knowledge of specific genetic mutations predisposing to PDAC may enable risk stratification, early detection, and the development of effective screening and surveillance programs. In the current study, the authors attempted to determine the diagnostic yield of testing for BRCA1/2 germline mutations in a PDAC screening cohort and a PDAC cohort referred for genetic testing.
Patients in a high-risk PDAC prevention and genetics program or those with a personal history of PDAC who were referred for genetic evaluation underwent testing for BRCA1/2 germline mutations. Clinical BRCA1/2 genetic testing included testing for the 3 Ashkenazi Jewish founder mutations or BRCA1/2 comprehensive testing.
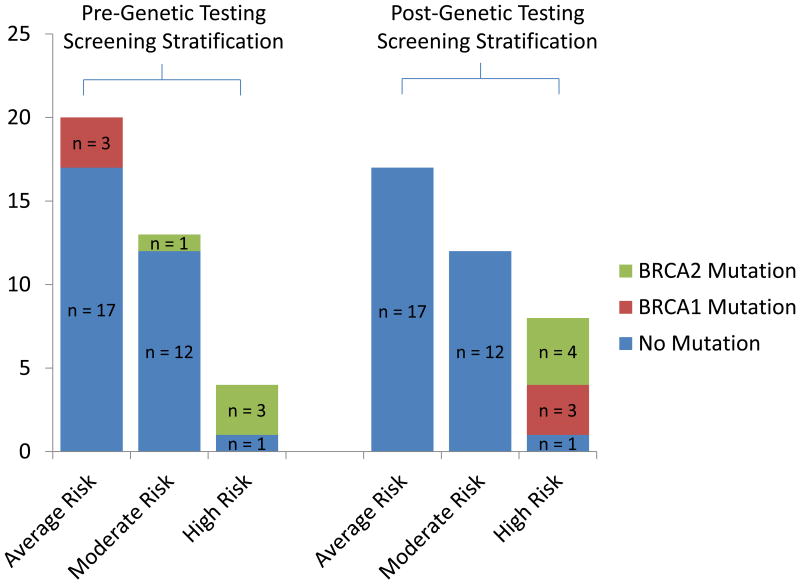
A total of 37 patients without PDAC underwent BRCA1/2 testing at the study institution. Genetic testing identified 7 patients who were BRCA1/2 carriers for a yield of 18.9%. Six patients carried Ashkenazi Jewish founder mutations (3 with BRCA1 and 3 with BRCA2), and 1 patient was found to have a BRCA2 mutation on comprehensive testing. Thirty-two patients with PDAC underwent BRCA1/2 genetic testing. Five patients had Ashkenazi Jewish founder mutations (2 with BRCA1 and 3 with BRCA2), and 2 patients were found to have BRCA2 mutations on comprehensive testing. The diagnostic yield was 7 of 32 patients (21.9%).
BRCA1/2 testing is useful in PDAC risk stratification and alters risk assignment and screening recommendations for mutation-positive patients and their families. Clinical BRCA1/2 testing should be considered in patients of Ashkenazi Jewish descent with a personal history or family history of PDAC, even in the absence of a family history of breast and ovarian cancer.
约10%的胰腺导管腺癌(PDAC)归因于遗传易感性,包括乳腺癌和卵巢癌综合征的种系突变BRCA1和BRCA2。了解导致PDAC的特定基因突变可能有助于进行风险分层、早期检测以及制定有效的筛查和监测计划。在本研究中,作者试图确定在一个PDAC筛查队列和一个因基因检测而转诊的PDAC队列中检测BRCA1/2种系突变的诊断率。
高危PDAC预防和遗传学项目中的患者或有PDAC个人病史且因基因评估而转诊的患者接受BRCA1/2种系突变检测。临床BRCA1/2基因检测包括检测3种阿什肯纳兹犹太奠基者突变或BRCA1/2全面检测。
共有37例无PDAC的患者在研究机构接受了BRCA1/2检测。基因检测确定了7例BRCA1/2携带者,检出率为18.9%。6例患者携带阿什肯纳兹犹太奠基者突变(3例为BRCA1,3例为BRCA2),1例患者在全面检测中发现有BRCA2突变。32例PDAC患者接受了BRCA1/2基因检测。5例患者有阿什肯纳兹犹太奠基者突变(2例为BRCA1,3例为BRCA2),2例患者在全面检测中发现有BRCA2突变。32例患者中的诊断率为7例(21.9%)。
BRCA1/2检测在PDAC风险分层中有用,并改变了突变阳性患者及其家族的风险评估和筛查建议。对于有PDAC个人病史或家族病史的阿什肯纳兹犹太裔患者,即使没有乳腺癌和卵巢癌家族史,也应考虑进行临床BRCA1/2检测。