Antonelli Andrea, Crimi Emanuele, Gobbi Alessandro, Torchio Roberto, Gulotta Carlo, Dellaca Raffaele, Scano Giorgio, Brusasco Vito, Pellegrino Riccardo
Allergologia e Fisiopatologia Respiratoria, ASO S. Croce e Carle, Cuneo, Italy.
Fisiopatologia Respiratoria, Dipartimento di Medicina Interna, Università di Genova, Genova, Italy.
Physiol Rep. 2013 Dec 8;1(7):e00166. doi: 10.1002/phy2.166. eCollection 2013 Dec 1.
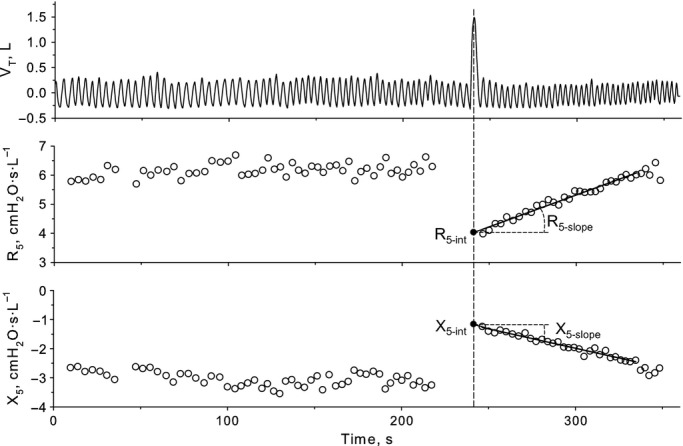
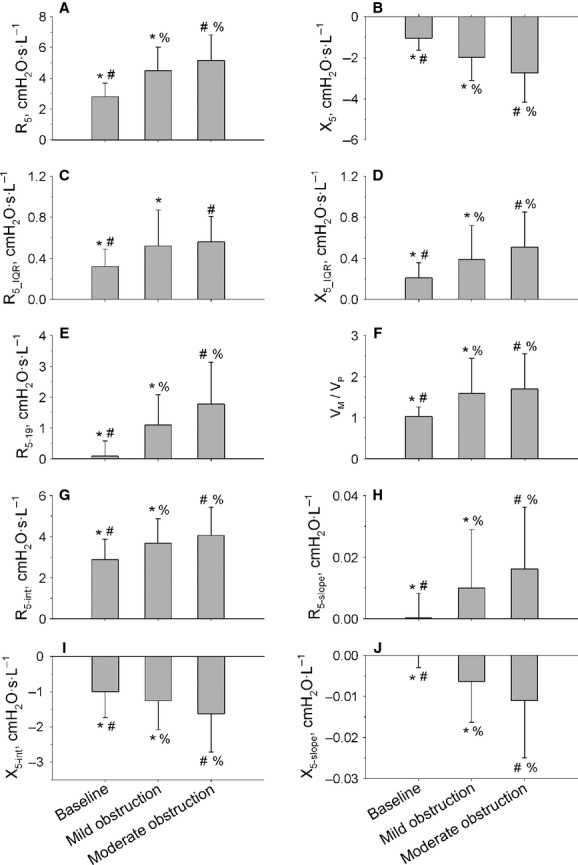
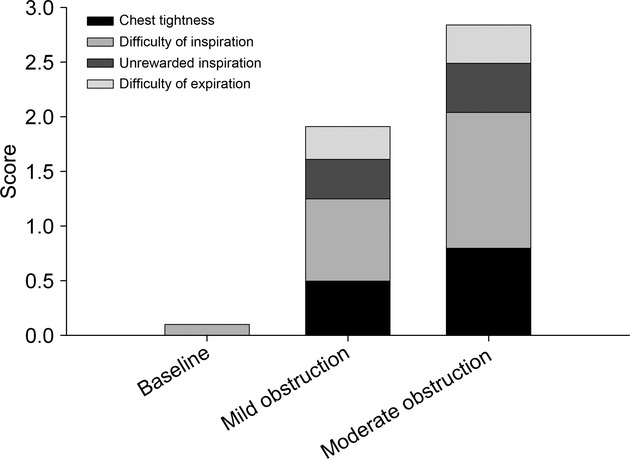
We hypothesized that dyspnea and its descriptors, that is, chest tightness, inspiratory effort, unrewarded inspiration, and expiratory difficulty in asthma reflect different mechanisms of airflow obstruction and their perception varies with the severity of bronchoconstriction. Eighty-three asthmatics were studied before and after inhalation of methacholine doses decreasing the 1-sec forced expiratory volume by ~15% (mild bronchoconstriction) and ~25% (moderate bronchoconstriction). Symptoms were examined as a function of changes in lung mechanics. Dyspnea increased with the severity of obstruction, mostly because of inspiratory effort and chest tightness. At mild bronchoconstriction, multivariate analysis showed that dyspnea was related to the increase in inspiratory resistance at 5 Hz (R 5) (r (2) = 0.10, P = 0.004), chest tightness to the decrease in maximal flow at 40% of control forced vital capacity, and the increase in R 5 at full lung inflation (r (2) = 0.15, P = 0.006), inspiratory effort to the temporal variability in R 5-19 (r (2) = 0.13, P = 0.003), and unrewarded inspiration to the recovery of R 5 after deep breath (r (2) = 0.07, P = 0.01). At moderate bronchoconstriction, multivariate analysis showed that dyspnea and inspiratory effort were related to the increase in temporal variability in inspiratory reactance at 5 Hz (X 5) (r (2) = 0.12, P = 0.04 and r (2) = 0.18, P < 0.001, respectively), and unrewarded inspiration to the decrease in X 5 at maximum lung inflation (r (2) = 0.07, P = 0.04). We conclude that symptom perception is partly explained by indexes of airway narrowing and loss of bronchodilatation with deep breath at low levels of bronchoconstriction, but by markers of ventilation heterogeneity and lung volume recruitment when bronchoconstriction becomes more severe.
我们假设,哮喘中的呼吸困难及其描述词,即胸闷、吸气用力、无效吸气和呼气困难,反映了气流阻塞的不同机制,且它们的感知会随支气管收缩的严重程度而变化。对83名哮喘患者在吸入不同剂量的乙酰甲胆碱前后进行了研究,这些剂量会使1秒用力呼气量分别降低约15%(轻度支气管收缩)和约25%(中度支气管收缩)。将症状作为肺力学变化的函数进行检查。呼吸困难随阻塞严重程度的增加而加重,主要是由于吸气用力和胸闷。在轻度支气管收缩时,多变量分析显示,呼吸困难与5赫兹时吸气阻力(R5)的增加有关(r(2)=0.10,P=0.004),胸闷与控制用力肺活量40%时最大流量的降低有关,以及与肺完全充气时R5的增加有关(r(2)=0.15,P=0.006),吸气用力与R5 - 19的时间变异性有关(r(2)=0.13,P=0.003),无效吸气与深呼吸后R5的恢复有关(r(2)=0.07,P=0.01)。在中度支气管收缩时,多变量分析显示,呼吸困难和吸气用力分别与5赫兹时吸气电抗(X5)的时间变异性增加有关(r(2)=0.12,P=0.04和r(2)=0.18,P<0.001),无效吸气与肺最大充气时X5的降低有关(r(2)=0.07,P=0.04)。我们得出结论,在支气管收缩程度较低时,症状感知部分可由气道狭窄和深呼吸时支气管扩张丧失的指标来解释,但当支气管收缩变得更严重时,则由通气异质性和肺容积募集的指标来解释。