Niëns Laurens M, Zelle Sten G, Gutiérrez-Delgado Cristina, Rivera Peña Gustavo, Hidalgo Balarezo Blanca Rosa, Rodriguez Steller Erick, Rutten Frans F H
Institute for Medical Technology Assessment and Institute for Health Policy & Management, Erasmus University Rotterdam, Rotterdam, The Netherlands.
Department of Primary and Community Care, Radboud University Nijmegen Medical Center, Nijmegen, The Netherlands.
PLoS One. 2014 Apr 25;9(4):e95836. doi: 10.1371/journal.pone.0095836. eCollection 2014.
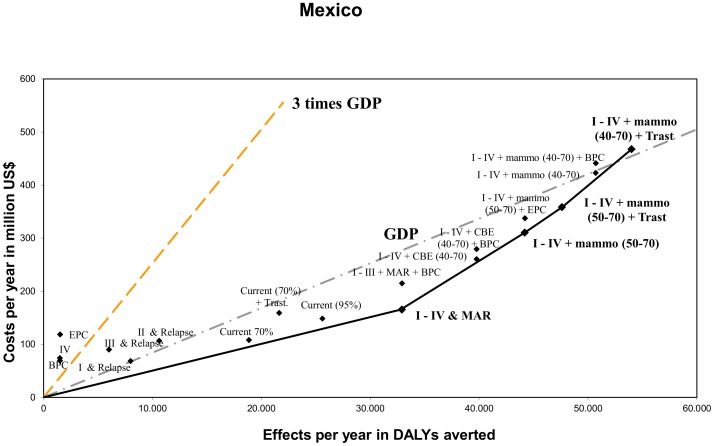
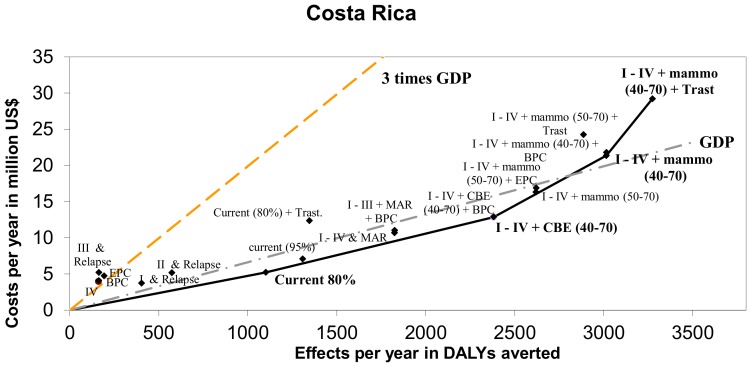
This paper reports the most cost-effective policy options to support and improve breast cancer control in Costa Rica and Mexico. Total costs and effects of breast cancer interventions were estimated using the health care perspective and WHO-CHOICE methodology. Effects were measured in disability-adjusted life years (DALYs) averted. Costs were assessed in 2009 United States Dollars (US$). To the extent available, analyses were based on locally obtained data. In Costa Rica, the current strategy of treating breast cancer in stages I to IV at a 80% coverage level seems to be the most cost-effective with an incremental cost-effectiveness ratio (ICER) of US$4,739 per DALY averted. At a coverage level of 95%, biennial clinical breast examination (CBE) screening could improve Costa Rica's population health twofold, and can still be considered very cost-effective (ICER US$5,964/DALY). For Mexico, our results indicate that at 95% coverage a mass-media awareness raising program (MAR) could be the most cost-effective (ICER US$5,021/DALY). If more resources are available in Mexico, biennial mammography screening for women 50-70 yrs (ICER US$12,718/DALY), adding trastuzumab (ICER US$13,994/DALY) or screening women 40-70 yrs biennially plus trastuzumab (ICER US$17,115/DALY) are less cost-effective options. We recommend both Costa Rica and Mexico to engage in MAR, CBE or mammography screening programs, depending on their budget. The results of this study should be interpreted with caution however, as the evidence on the intervention effectiveness is uncertain. Also, these programs require several organizational, budgetary and human resources, and the accessibility of breast cancer diagnostic, referral, treatment and palliative care facilities should be improved simultaneously. A gradual implementation of early detection programs should give the respective Ministries of Health the time to negotiate the required budget, train the required human resources and understand possible socioeconomic barriers.
本文报告了在哥斯达黎加和墨西哥支持并改善乳腺癌防治工作的最具成本效益的政策选择。采用卫生保健视角和世界卫生组织-CHOICE方法估算了乳腺癌干预措施的总成本和效果。效果以避免的伤残调整生命年(DALYs)衡量。成本以2009年美元(US$)评估。在可行的范围内,分析基于当地获取的数据。在哥斯达黎加,目前以80%的覆盖率对I至IV期乳腺癌进行治疗的策略似乎最具成本效益,每避免一个DALY的增量成本效益比(ICER)为4739美元。在95%的覆盖率水平下,两年一次的临床乳腺检查(CBE)筛查可使哥斯达黎加的人群健康改善两倍,且仍可被视为极具成本效益(ICER为5964美元/DALY)。对于墨西哥,我们的结果表明,在95%的覆盖率下,大众媒体提高认识计划(MAR)可能最具成本效益(ICER为5021美元/DALY)。如果墨西哥有更多资源,对50 - 70岁女性进行两年一次的乳腺钼靶筛查(ICER为12718美元/DALY)、添加曲妥珠单抗(ICER为13994美元/DALY)或对40 - 70岁女性进行两年一次的筛查并添加曲妥珠单抗(ICER为17115美元/DALY)是成本效益较低的选择。我们建议哥斯达黎加和墨西哥根据各自预算开展大众媒体提高认识计划、临床乳腺检查或乳腺钼靶筛查项目。然而,本研究结果应谨慎解读,因为干预效果的证据尚不确定。此外,这些项目需要若干组织、预算和人力资源,同时应改善乳腺癌诊断、转诊、治疗和姑息治疗设施的可及性。早期检测项目的逐步实施应使各国卫生部有时间协商所需预算、培训所需人力资源并了解可能的社会经济障碍。