Beggs Andrew D, Dilworth Mark P, Powell Susan L, Atherton Helen, Griffiths Ewen A
Academic Department of Surgery, School of Cancer Sciences, University of Birmingham, Birmingham, UK.
Department of Geriatric Medicine, Heart of England NHS Foundation Trust, Solihull Hospital, Birmingham, UK.
Clin Exp Gastroenterol. 2014 Apr 16;7:93-104. doi: 10.2147/CEG.S56725. eCollection 2014.
Emergency surgery or transarterial embolization (TAE) are options for the treatment of recurrent or refractory nonvariceal upper gastrointestinal bleeding. Surgery has the disadvantage of high rates of postoperative morbidity and mortality. Embolization has become more available and has the advantage of avoiding laparotomy in this often unfit and elderly population.
To carry out a systematic review and meta-analysis of all studies that have directly compared TAE with emergency surgery in the treatment of major upper gastrointestinal bleeding that has failed therapeutic upper gastrointestinal endoscopy.
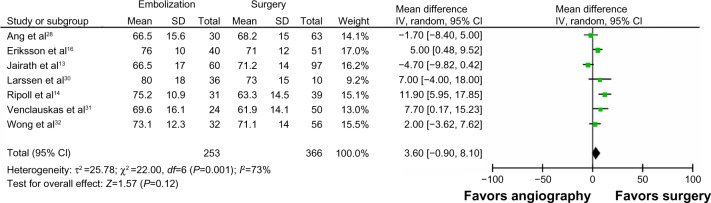
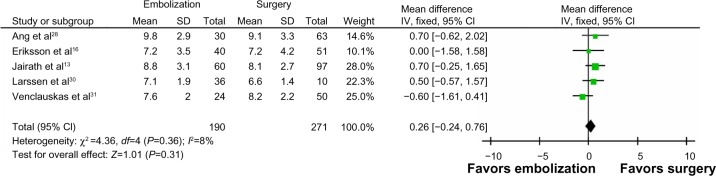
A literature search of Ovid MEDLINE, Embase, and Google Scholar was performed. The primary outcomes were all-cause mortality and rates of rebleeding. The secondary outcomes were length of stay and postoperative complications.
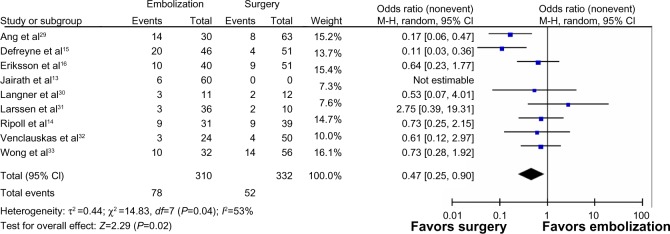
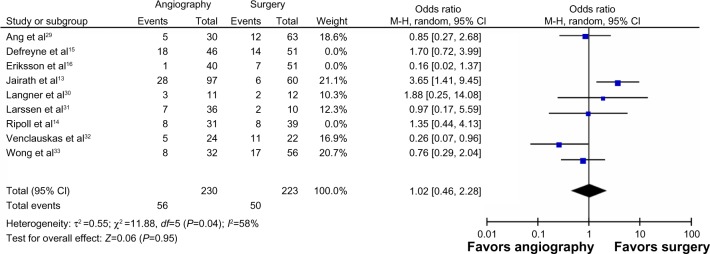
A total of nine studies with 711 patients (347 who had embolization and 364 who had surgery) were analyzed. Patients in the TAE group were more likely to have ischemic heart disease (odds ratio [OR] =1.99; 95% confidence interval [CI]: 1.33, 2.98; P=0.0008; I (2)=67% [random effects model]) and be coagulopathic (pooled OR =2.23; 95% CI: 1.29, 3.87; P=0.004; I (2)=33% [fixed effects model]). Compared with TAE, surgery was associated with a lower risk of rebleeding (OR =0.41; 95% CI: 0.22, 0.77; P<0.0001; I (2)=55% [random effects]). There was no difference in mortality (OR =0.70; 95% CI: 0.48, 1.02; P=0.06; I (2)=44% [fixed effects]) between TAE and surgery.
When compared with surgery, TAE had a significant increased risk of rebleeding rates after TAE; however, there were no differences in mortality rates. These findings are subject to multiple sources of bias due to poor quality studies. These findings support the need for a well-designed clinical trial to ascertain which technique is superior.
急诊手术或经动脉栓塞术(TAE)是治疗复发性或难治性非静脉曲张性上消化道出血的选择。手术的缺点是术后发病率和死亡率较高。在这类通常身体状况不佳的老年人群中,栓塞术应用更为广泛,且具有避免开腹手术的优势。
对所有直接比较TAE与急诊手术治疗经治疗性上消化道内镜检查失败的严重上消化道出血的研究进行系统评价和荟萃分析。
检索了Ovid MEDLINE、Embase和谷歌学术。主要结局为全因死亡率和再出血率。次要结局为住院时间和术后并发症。
共分析了9项研究,涉及711例患者(347例行栓塞术,364例行手术)。TAE组患者更易患缺血性心脏病(比值比[OR]=1.99;95%置信区间[CI]:1.33,2.98;P=0.0008;I²=67%[随机效应模型])且存在凝血功能障碍(合并OR=2.23;95%CI:1.29,3.87;P=0.004;I²=33%[固定效应模型])。与TAE相比,手术再出血风险较低(OR=0.41;95%CI:0.22,0.77;P<0.0001;I²=55%[随机效应])。TAE与手术在死亡率方面无差异(OR=0.70;95%CI:0.48,1.02;P=0.06;I²=44%[固定效应])。
与手术相比,TAE术后再出血率风险显著增加;然而,死亡率无差异。由于研究质量较差,这些结果存在多种偏倚来源。这些结果支持需要进行一项设计良好的临床试验以确定哪种技术更具优势。