Silverman Michael G, Harkness James R, Blankstein Ron, Budoff Matthew J, Agatston Arthur S, Carr J Jeffrey, Lima Joao A, Blumenthal Roger S, Nasir Khurram, Blaha Michael J
Johns Hopkins Ciccarone Center for Prevention of Heart Disease, Baltimore, MD.
Brigham and Women's Hospital, Boston MA.
JACC Cardiovasc Imaging. 2014 May;7(5):476-486. doi: 10.1016/j.jcmg.2014.03.005.
The aim of this study was to evaluate the impact of coronary artery calcium (CAC) burden and regional distribution on the need for and type of future coronary revascularization-percutaneous versus surgical (coronary artery bypass graft [CABG])-among asymptomatic subjects.
The need for coronary revascularization and the chosen mode of revascularization are thought to be functions of disease burden and anatomic distribution. The association between the baseline burden and regional distribution of CAC and the risk and type of future coronary revascularization remains unknown.
A total of 6,540 participants in the MESA (Multi-Ethnic Study of Atherosclerosis) (subjects aged 45 to 84 years, free of known baseline cardiovascular disease) with vessel-specific CAC measurements were followed for a median of 8.5 years (interquartile range: 7.7 to 8.6 years). Annualized rates and multivariate-adjusted hazard ratios for revascularization and revascularization type were analyzed according to CAC score category, number of vessels with CAC (0 to 4, including the left main coronary artery), and involvement of individual coronary arteries.
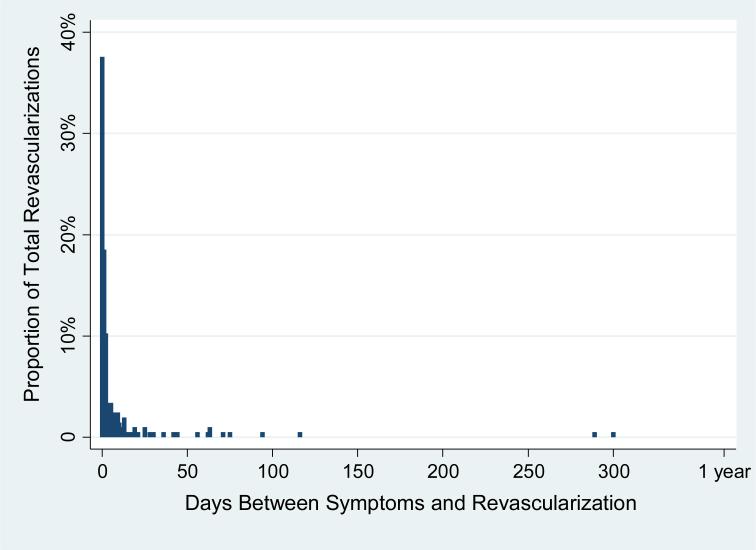
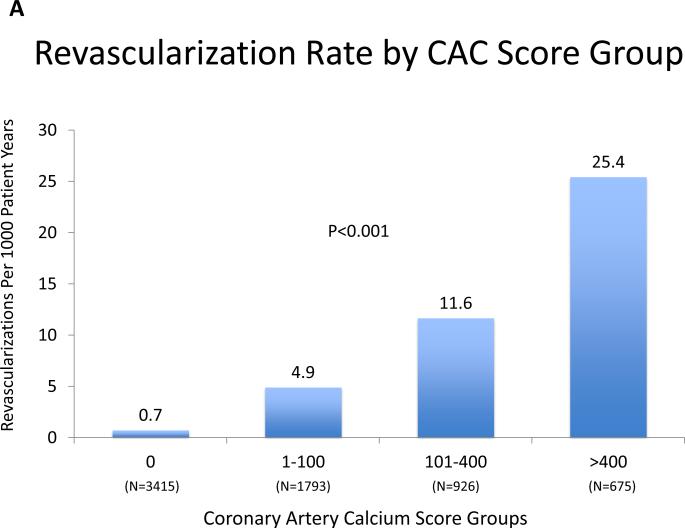
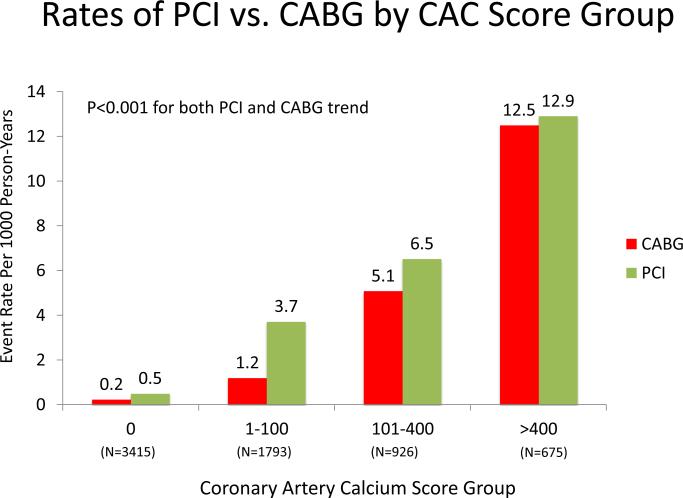
A total of 265 revascularizations (4.2%) occurred during follow-up, and 206 (78% of the total) were preceded by adjudicated symptoms. Revascularization was uncommon when CAC score was 0.0 (0.6%), with a graded increase over both rising CAC burden and increasingly diffuse CAC distribution. The revascularization rates per 1,000 person-years for CAC scores of 1 to 100, 101 to 400, and >400 were 4.9, 11.7, and 25.4, respectively; for 1, 2, 3, and 4 vessels with CAC, the rates were 3.0, 8.0, 16.1, and 24.8, respectively. In multivariate models adjusting for CAC score, the number of vessels with CAC remained predictive of revascularization and mode of revascularization. Independent predictors of CABG versus percutaneous coronary intervention included 3- or 4-vessel CAC, higher CAC burden, and involvement of the left main coronary artery. Risk for CABG was extremely low with <3-vessel baseline CAC. Results were similar when considering only symptom-driven revascularizations.
In this multiethnic cohort of asymptomatic subjects, baseline CAC was highly predictive of future coronary revascularization procedures, with measures of CAC burden and distribution each independently predicting need for percutaneous coronary intervention versus CABG over an 8.5-year follow-up.
本研究旨在评估冠状动脉钙化(CAC)负荷和区域分布对无症状受试者未来冠状动脉血运重建需求及类型(经皮介入与外科手术,即冠状动脉旁路移植术[CABG])的影响。
冠状动脉血运重建的需求及所选的血运重建方式被认为是疾病负荷和解剖分布的函数。CAC的基线负荷和区域分布与未来冠状动脉血运重建的风险及类型之间的关联仍不清楚。
对多民族动脉粥样硬化研究(MESA)中6540名参与者(年龄45至84岁,无已知的基线心血管疾病)进行血管特异性CAC测量,随访时间中位数为8.5年(四分位间距:7.7至8.6年)。根据CAC评分类别、存在CAC的血管数量(0至4支,包括左主干冠状动脉)以及各冠状动脉的受累情况,分析血运重建的年化率和多变量调整后的风险比以及血运重建类型。
随访期间共发生265例血运重建(4.2%),其中206例(占总数的78%)有经判定的症状。当CAC评分为0.0时,血运重建不常见(0.6%),随着CAC负荷增加和CAC分布越来越弥散,血运重建发生率呈梯度上升。CAC评分为1至100、101至400和>400时,每1000人年的血运重建率分别为4.9、11.7和25.4;存在1、2、3和4支有CAC的血管时,血运重建率分别为3.0、8.0、16.1和24.8。在调整了CAC评分的多变量模型中,存在CAC的血管数量仍然是血运重建及血运重建方式的预测指标。CABG与经皮冠状动脉介入治疗的独立预测因素包括3支或4支血管存在CAC、较高的CAC负荷以及左主干冠状动脉受累。基线存在<3支血管的CAC时,CABG的风险极低。仅考虑症状驱动的血运重建时,结果相似。
在这个多民族无症状受试者队列中,基线CAC对未来冠状动脉血运重建手术具有高度预测性,在8.5年的随访中,CAC负荷和分布的测量指标各自独立预测经皮冠状动脉介入治疗与CABG的需求。