Blaha Michael J, Budoff Matthew J, Tota-Maharaj Rajesh, Dardari Zeina A, Wong Nathan D, Kronmal Richard A, Eng John, Post Wendy S, Blumenthal Roger S, Nasir Khurram
Johns Hopkins Ciccarone Center for the Prevention of Heart Disease, Baltimore, Maryland.
Division of Cardiology, Los Angeles Biomedical Research Institute at Harbor-UCLA, Torrance, California.
JACC Cardiovasc Imaging. 2016 Dec;9(12):1407-1416. doi: 10.1016/j.jcmg.2016.03.001. Epub 2016 Apr 13.
The aim of this study was to investigate whether inclusion of simple measures of calcified plaque distribution might improve the ability of the traditional Agatston coronary artery calcium (CAC) score to predict cardiovascular events.
Agatston CAC scoring does not include information on the location and distributional pattern of detectable calcified plaque.
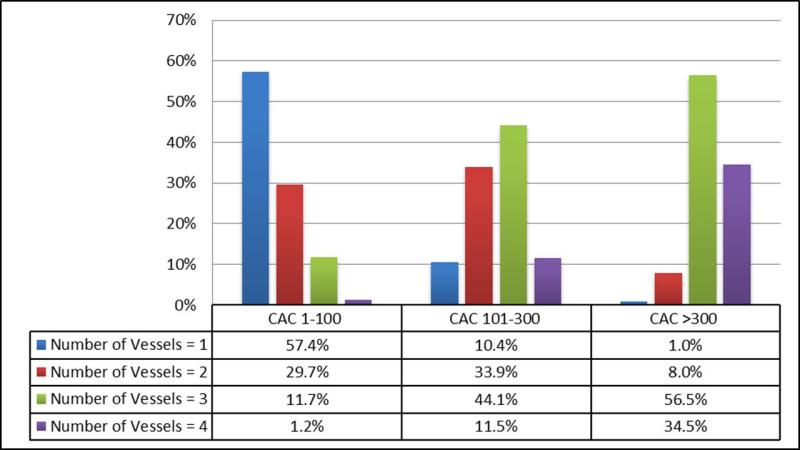
We studied 3,262 (50%) individuals with baseline CAC >0 from MESA (Multi-Ethnic Study of Atherosclerosis). Multivessel CAC was defined by the number of coronary vessels with CAC (scored 1 to 4, including the left main). The "diffusivity index" was calculated as: 1 - (CAC in most affected vessel/total CAC), and was used to group participants into concentrated and diffuse CAC patterns. Multivariable Cox proportional hazards regression, area under the curve, and net reclassification improvement analyses were performed for both coronary heart disease (CHD) and cardiovascular disease (CVD) events to assess whether measures of regional CAC distribution add to the traditional Agatston CAC score.
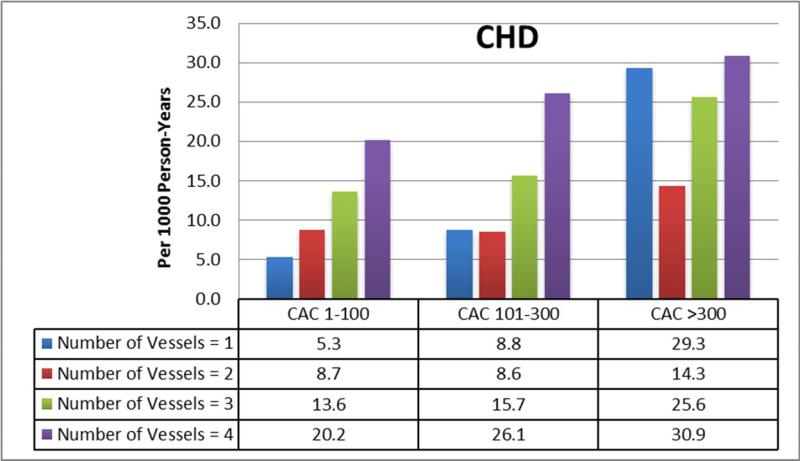
Mean age of the population was 66 ± 10 years, with 42% women. Median follow-up was 10.0 (9.5 to 10.7) years and there were 368 CHD and 493 CVD events during follow-up. Considerable heterogeneity existed between CAC score group and number of vessels with CAC (p < 0.01). Addition of number of vessels with CAC significantly improved capacity to predict CHD and CVD events in survival analysis (hazard ratio: 1.9 to 3.5 for 4-vessel vs. 1-vessel CAC), area under the curve analysis (C-statistic improvement of 0.01 to 0.033), and net reclassification improvement analysis (category-less net reclassification improvement 0.10 to 0.45). Although a diffuse CAC pattern was associated with worse outcomes in participants with ≥2 vessels with CAC (hazard ratio: 1.33 to 1.41; p < 0.05), adding this variable to the Agatston CAC score and number of vessels with CAC did not further improve global risk prediction.
The number of coronary arteries with calcified plaque, indicating increasingly "diffuse" multivessel subclinical atherosclerosis, adds significantly to the traditional Agatston CAC score for the prediction of CHD and CVD events.
本研究旨在探讨纳入钙化斑块分布的简单测量指标是否能提高传统阿加斯顿冠状动脉钙化(CAC)评分预测心血管事件的能力。
阿加斯顿CAC评分未包含可检测到的钙化斑块的位置和分布模式信息。
我们研究了动脉粥样硬化多族裔研究(MESA)中3262名(50%)基线CAC>0的个体。多支血管CAC由存在CAC的冠状动脉数量定义(评分为1至4,包括左主干)。“扩散指数”计算为:1 - (最严重受累血管的CAC/总CAC),并用于将参与者分为集中型和弥漫型CAC模式。对冠心病(CHD)和心血管疾病(CVD)事件进行多变量Cox比例风险回归、曲线下面积和净重新分类改善分析,以评估区域CAC分布测量指标是否能补充传统阿加斯顿CAC评分。
研究人群的平均年龄为66±10岁,女性占42%。中位随访时间为10.0(9.5至10.7)年,随访期间有368例CHD事件和493例CVD事件。CAC评分组与存在CAC的血管数量之间存在显著异质性(p<0.01)。在生存分析中,添加存在CAC的血管数量显著提高了预测CHD和CVD事件的能力(风险比:4支血管CAC与1支血管CAC相比为1.9至3.5)、曲线下面积分析(C统计量改善0.01至0.033)以及净重新分类改善分析(无类别净重新分类改善0.10至0.45)。尽管在存在≥2支血管CAC的参与者中,弥漫型CAC模式与更差的结局相关(风险比:1.33至1.41;p<0.05),但将该变量添加到阿加斯顿CAC评分和存在CAC的血管数量中并未进一步改善总体风险预测。
存在钙化斑块的冠状动脉数量表明多支血管亚临床动脉粥样硬化日益“弥漫”,在预测CHD和CVD事件方面,显著补充了传统阿加斯顿CAC评分。