Generali D, Buffa F M, Deb S, Cummings M, Reid L E, Taylor M, Andreis D, Allevi G, Ferrero G, Byrne D, Martinotti M, Bottini A, Harris A L, Lakhani S R, Fox S B
US Terapia Molecolare e Farmacogenomica/UO Chirurgia Generale Senologica, AO Istituti Ospitalieri di Cremona, Viale Concordia 1, 26100 Cremona, Italy.
Molecular Oncology Laboratories, Weatherall Institute of Molecular Medicine, University of Oxford, John Radcliffe Hospital, Oxford OX3 9DS, UK.
Br J Cancer. 2014 Jul 8;111(1):46-54. doi: 10.1038/bjc.2014.236. Epub 2014 May 29.
Stratification of patients for treatment of ductal carcinoma in situ (DCIS) is suboptimal, with high systemic overtreatment rates.
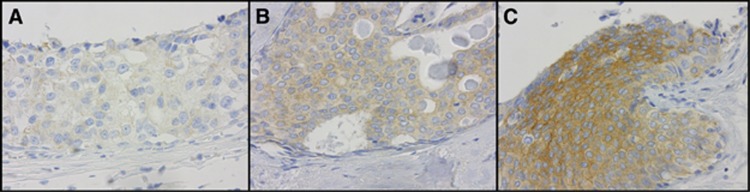
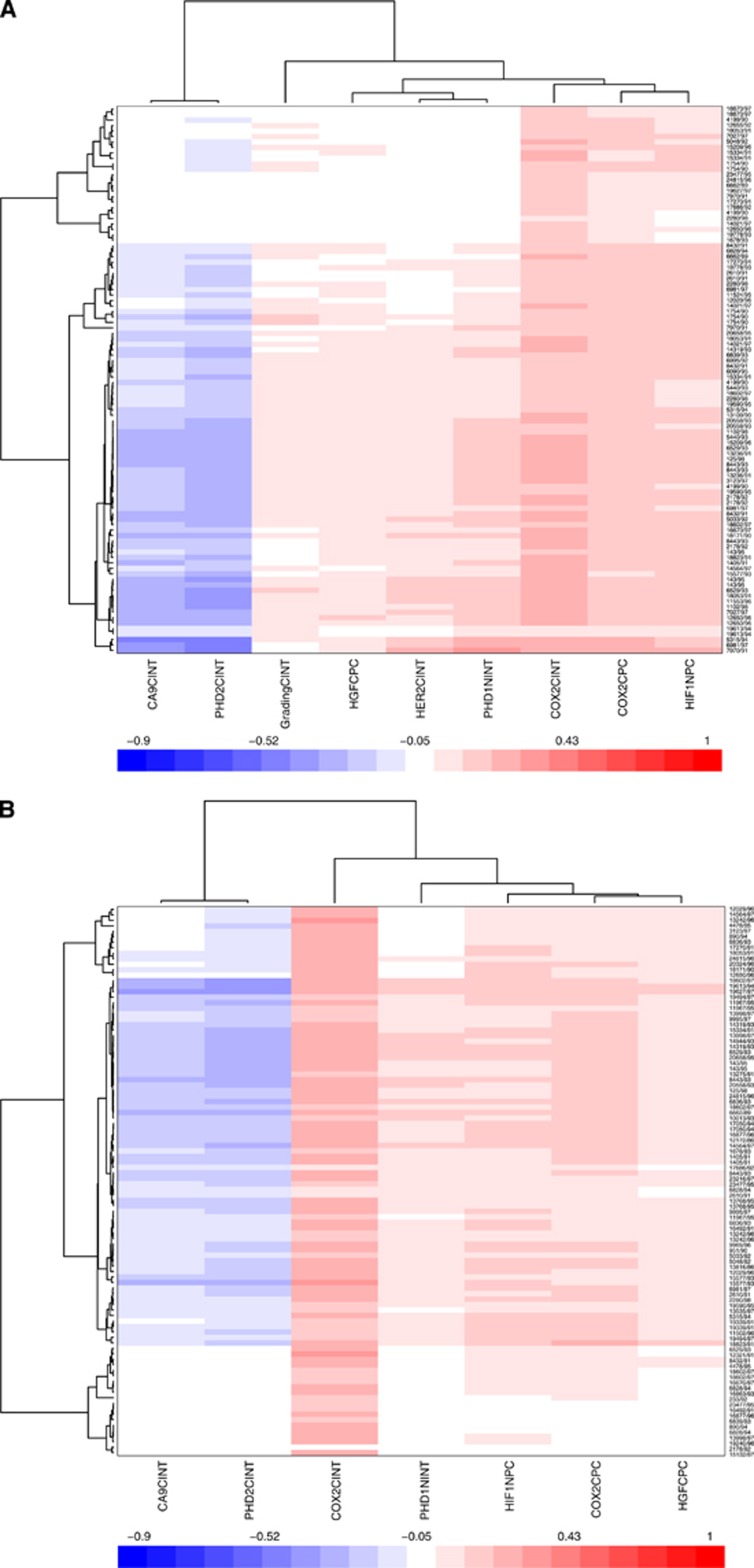
A training set of 95 tumours from women with pure DCIS were immunostained for proteins involved in cell survival, hypoxia, growth factor and hormone signalling. A generalised linear regression with regularisation and variable selection was applied to a multiple covariate Cox survival analysis with recurrence-free survival 10-fold cross-validation and leave-one-out iterative approach were used to build and test the model that was validated using an independent cohort of 58 patients with pure DCIS. The clinical role of a COX-2-targeting agent was then tested in a proof-of-concept neoadjuvant randomised trial in ER-positive DCIS treated with exemestane 25 mg day(-1)± celecoxib 800 mg day(-1).
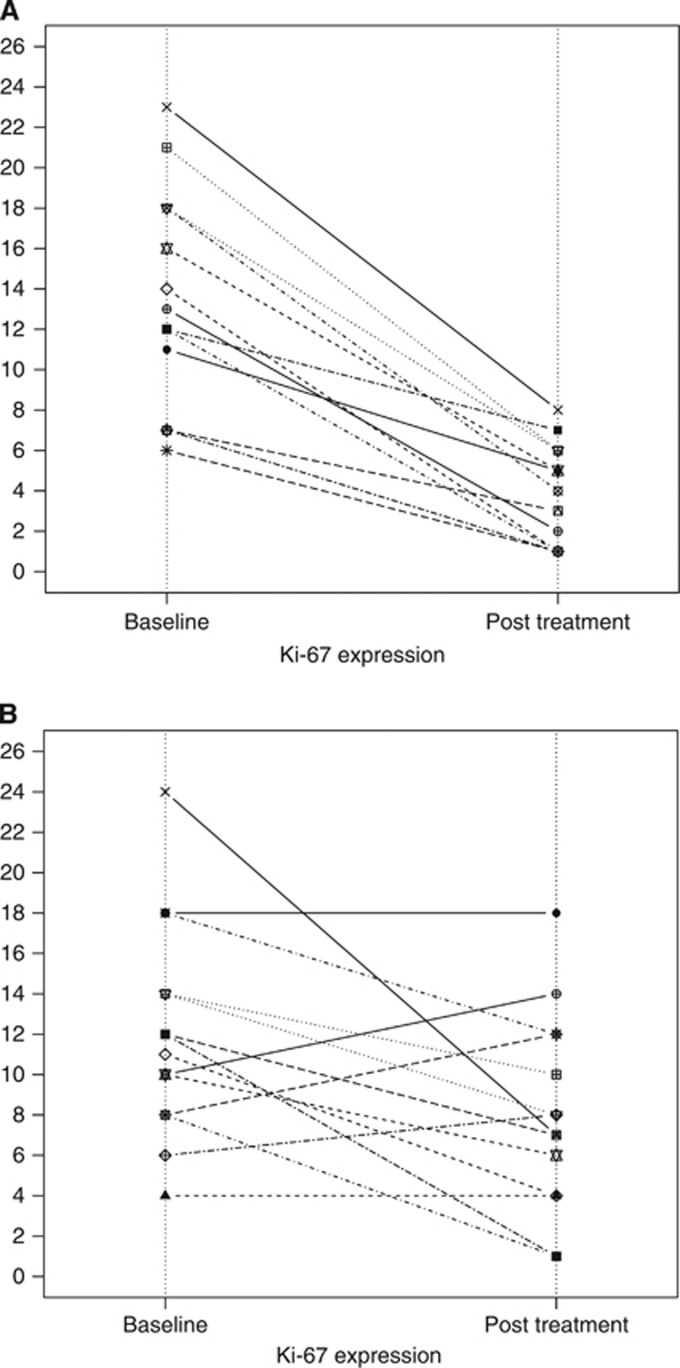
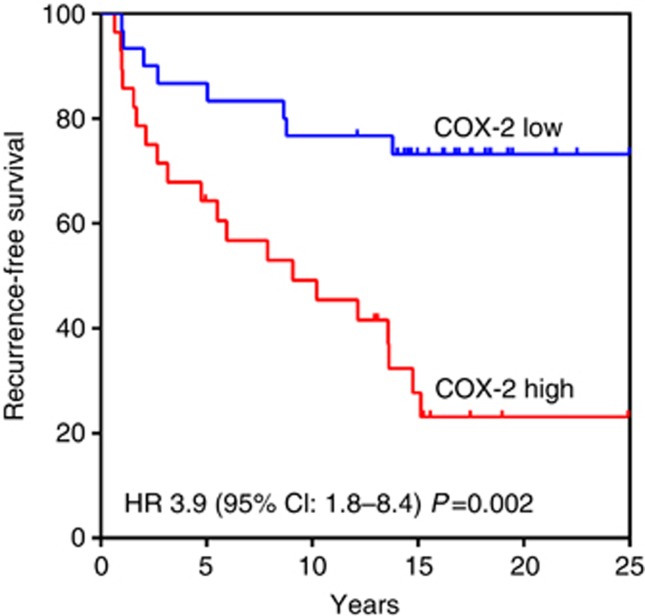
The COX-2 expression was an independent prognostic factor for early relapse in the training (HR 37.47 (95% CI: 5.56-252.74) P=0.0001) and independent validation cohort (HR 3.9 (95% CI: 1.8-8.3) P=0.002). There was no significant interaction with other clinicopathological variables. A statistically significant reduction of Ki-67 expression after treatment with exemestane ± celecoxib was observed (P<0.02) with greater reduction in the combination arm (P<0.004). Concomitant reduction in COX-2 expression was statistically significant in the exemestane and celecoxib arm (P<0.03) only.
In patients with DCIS, COX-2 may predict recurrence, aiding clinical decision making. A combination of an aromatase inhibitor and celecoxib has significant biological effect and may be integrated into treatment of COX2-positive DCIS at high risk of recurrence.
导管原位癌(DCIS)患者的分层治疗效果欠佳,存在较高的全身过度治疗率。
对95例纯DCIS女性患者的肿瘤进行免疫染色,检测与细胞存活、缺氧、生长因子和激素信号传导相关的蛋白质。将带有正则化和变量选择的广义线性回归应用于多协变量Cox生存分析,采用无复发生存10倍交叉验证和留一法迭代方法构建并测试模型,该模型在58例纯DCIS独立队列中进行验证。然后,在一项概念验证性新辅助随机试验中,对25 mg/天依西美坦±800 mg/天塞来昔布治疗的雌激素受体(ER)阳性DCIS患者,测试COX-2靶向药物的临床作用。
在训练队列(风险比[HR] 37.47,95%置信区间[CI]:5.56 - 252.74,P = 0.0001)和独立验证队列(HR 3.9,95% CI:1.8 - 8.3,P = 0.002)中,COX-2表达是早期复发的独立预后因素。与其他临床病理变量无显著交互作用。观察到依西美坦±塞来昔布治疗后Ki-67表达有统计学显著降低(P < 0.02),联合治疗组降低更明显(P < 0.004)。仅在依西美坦和塞来昔布联合治疗组中观察到COX-2表达的伴随降低有统计学意义(P < 0.03)。
在DCIS患者中,COX-2可能预测复发,有助于临床决策。芳香化酶抑制剂和塞来昔布联合使用具有显著生物学效应,可纳入复发高危的COX2阳性DCIS的治疗。