Kok Victor C, Horng Jorng-Tzong, Chang Wan-Shan, Hong Ya-Fang, Chang Tzu-Hao
Public Health and Clinical Informatics Research Group, Department of Biomedical Informatics, Asia University, Wufeng, Taichung, Taiwan; Department of Internal Medicine, Kuang Tien General Hospital, Shalu, Taichung, Taiwan.
Public Health and Clinical Informatics Research Group, Department of Biomedical Informatics, Asia University, Wufeng, Taichung, Taiwan; Department of Computer Science and Information Engineering, National Central University, Jhongli, Taoyuan, Taiwan.
PLoS One. 2014 Jun 4;9(6):e99102. doi: 10.1371/journal.pone.0099102. eCollection 2014.
Previous studies have shown an association between gout and/or hyperuricemia and a subsequent increase in cardiovascular disease (CVD) outcomes. Allopurinol reduces vascular oxidative stress, ameliorates inflammatory state, improves endothelial function, and prevents atherosclerosis progression. Accordingly, we tested the hypothesis that a positive association between allopurinol therapy in gout patients and future cardiovascular outcomes is present using a population-based matched-cohort study design.
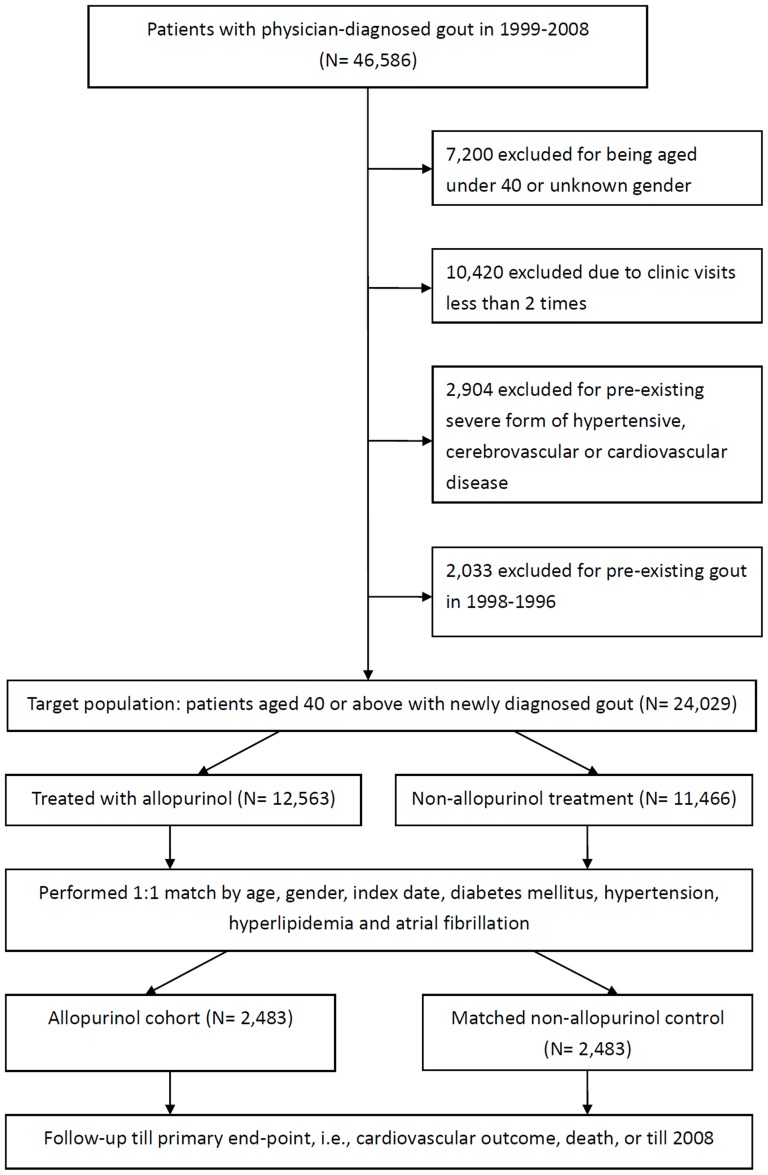
Patients aged ≥40 years with newly diagnosed gout having no pre-existing severe form of CVD were separated into allopurinol (n = 2483) and non-allopurinol (n = 2483) groups after matching for age, gender, index date, diabetes mellitus, hypertension, hyperlipidemia, and atrial fibrillation. The two groups were also balanced in terms of uric acid nephrolithiasis, acute kidney injury, hepatitis, and Charlson comorbidity index.
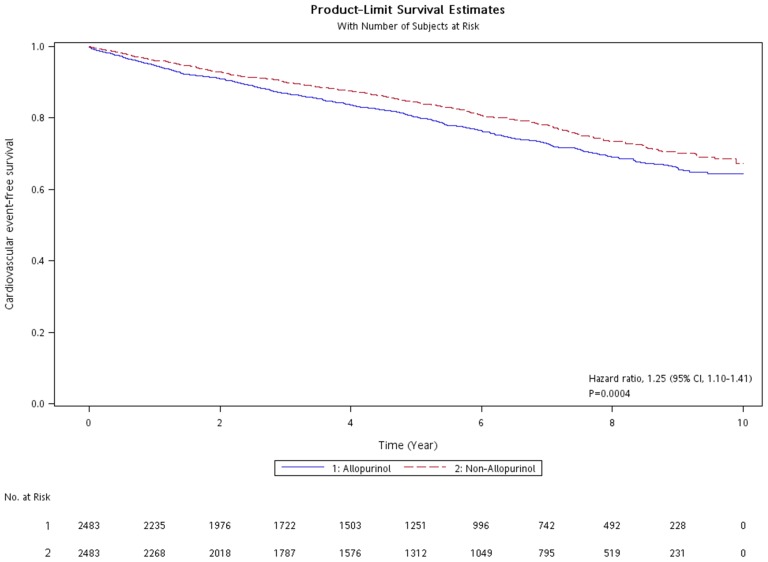
With a median follow-up time of 5.25 years, the allopurinol group had a modest increase in cardiovascular risk [relative risk, 1.20; 95% confidence interval (CI), 1.08-1.34]. A Cox proportional hazard model adjusted for chronic kidney disease, uremia, and gastric ulcer gave a hazard ratio (HR) for cardiovascular outcomes of 1.25 (95% CI, 1.10-1.41) in gout patients receiving allopurinol compared with the non-allopurinol group. In further analysis of patients receiving urate-lowering therapy, the uricosuric agent group (n = 1713) had an adjusted HR of 0.83 (0.73-0.95) for cardiovascular events compared with the allopurinol group.
The current population-based matched-cohort study did not support the association between allopurinol therapy in gout patients with normal risk for cardiovascular sequels and beneficial future cardiovascular outcomes. Several important risk factors for cardiovascular disease, such as smoking, alcohol consumption, body mass index, blood pressure were not obtainable in the current retrospective cohort study, thus could potentially bias the effect estimate.
既往研究表明痛风和/或高尿酸血症与随后心血管疾病(CVD)结局增加之间存在关联。别嘌醇可降低血管氧化应激、改善炎症状态、改善内皮功能并防止动脉粥样硬化进展。因此,我们采用基于人群的匹配队列研究设计,检验了痛风患者接受别嘌醇治疗与未来心血管结局之间存在正相关的假设。
年龄≥40岁、新诊断为痛风且无既往严重形式CVD的患者,在根据年龄、性别、索引日期、糖尿病、高血压、高脂血症和心房颤动进行匹配后,分为别嘌醇组(n = 2483)和非别嘌醇组(n = 2483)。两组在尿酸肾结石、急性肾损伤、肝炎和查尔森合并症指数方面也保持平衡。
中位随访时间为5.25年,别嘌醇组心血管风险略有增加[相对风险,1.20;95%置信区间(CI),1.08 - 1.34]。在对慢性肾病、尿毒症和胃溃疡进行校正的Cox比例风险模型中,接受别嘌醇治疗的痛风患者与非别嘌醇组相比,心血管结局的风险比(HR)为1.25(95%CI,1.10 - 1.41)。在对接受降尿酸治疗的患者进行进一步分析时,促尿酸排泄剂组(n = 1713)与别嘌醇组相比,心血管事件的校正HR为0.83(0.73 - 0.95)。
当前基于人群的匹配队列研究不支持痛风患者接受别嘌醇治疗与未来有益的心血管结局之间的关联,这些痛风患者发生心血管后遗症的风险正常。在当前的回顾性队列研究中,无法获得一些重要的心血管疾病风险因素,如吸烟、饮酒、体重指数、血压,因此可能会使效应估计产生偏差。