Abou Chakra Claire Nour, Pepin Jacques, Sirard Stephanie, Valiquette Louis
Department of Microbiology and Infectious Diseases, Université de Sherbrooke, Sherbrooke, Quebec, Canada.
PLoS One. 2014 Jun 4;9(6):e98400. doi: 10.1371/journal.pone.0098400. eCollection 2014.
Clostridium difficile infection (CDI) can lead to complications, recurrence, and death. Numerous studies have assessed risk factors for these unfavourable outcomes, but systematic reviews or meta-analyses published so far were limited in scope or in quality.
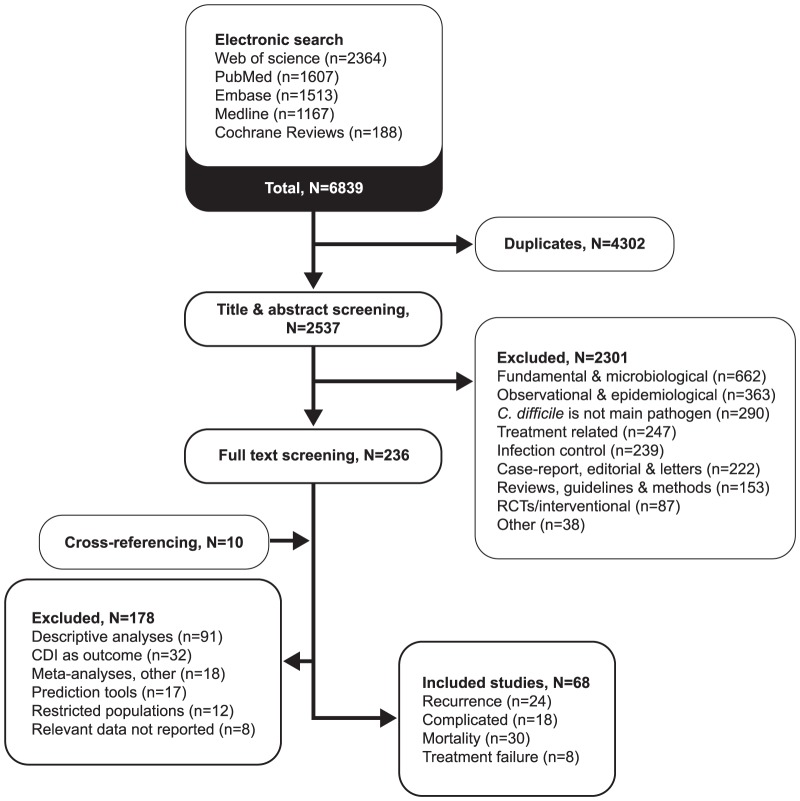
A systematic review was completed according to PRISMA guidelines. An electronic search in five databases was performed. Studies published until October 2013 were included if risk factors for at least one CDI outcome were assessed with multivariate analyses.
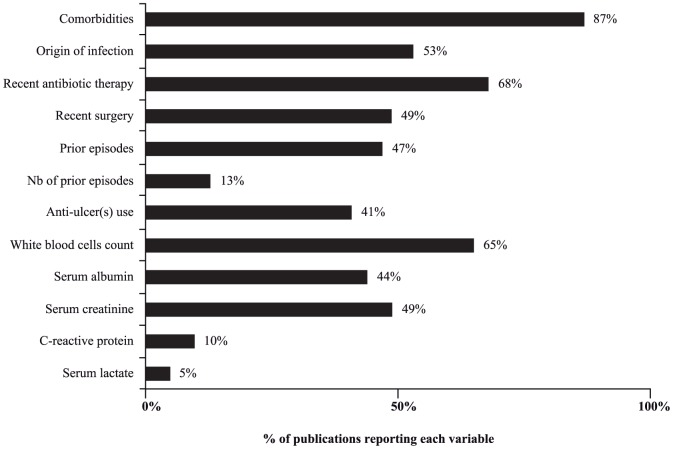
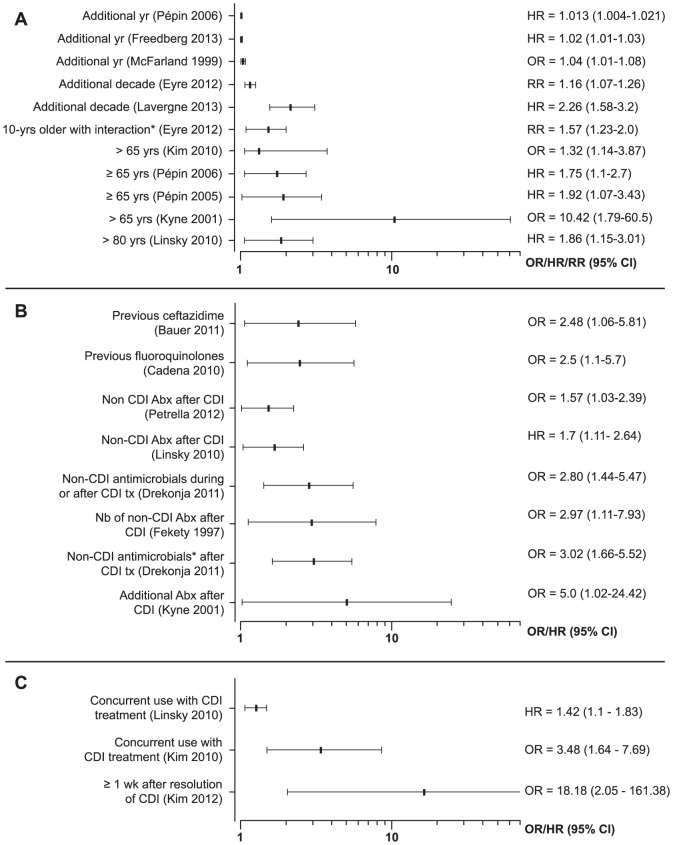
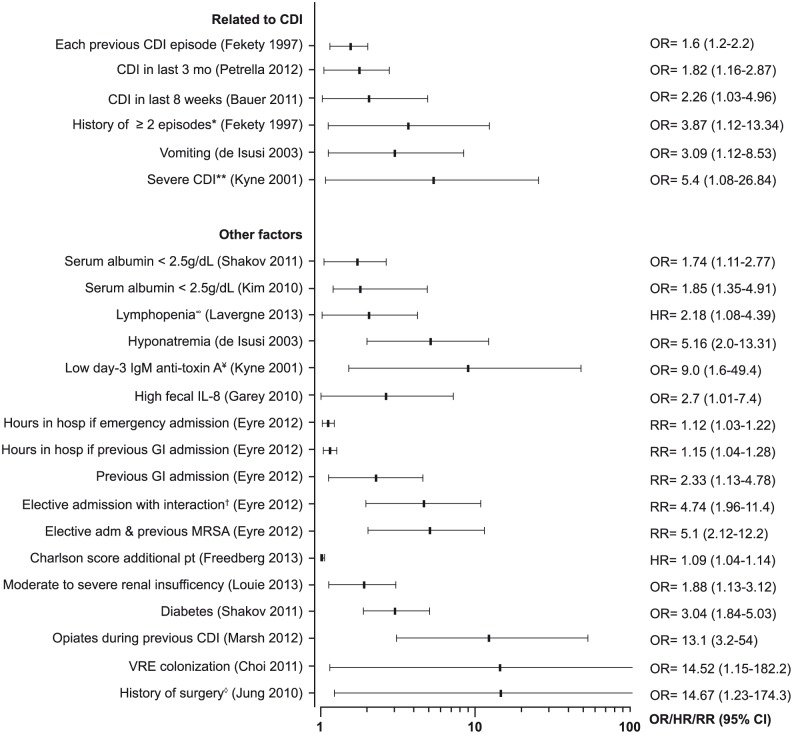
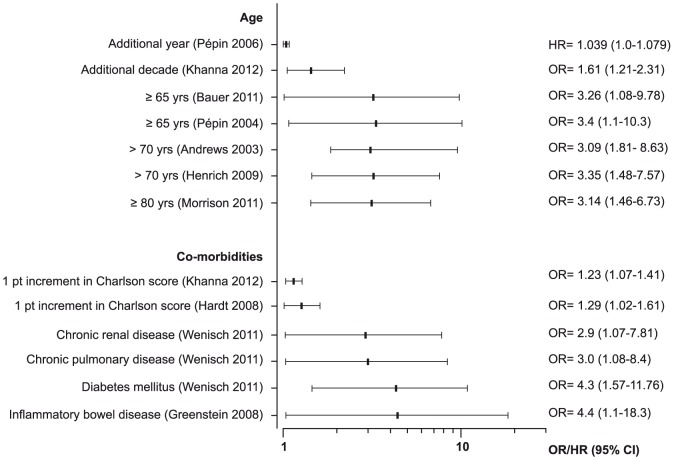
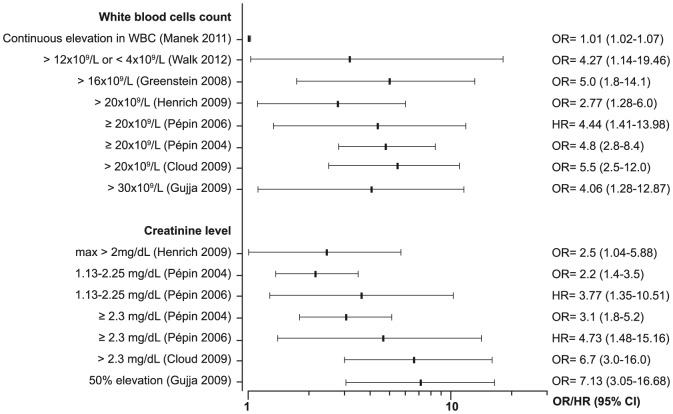
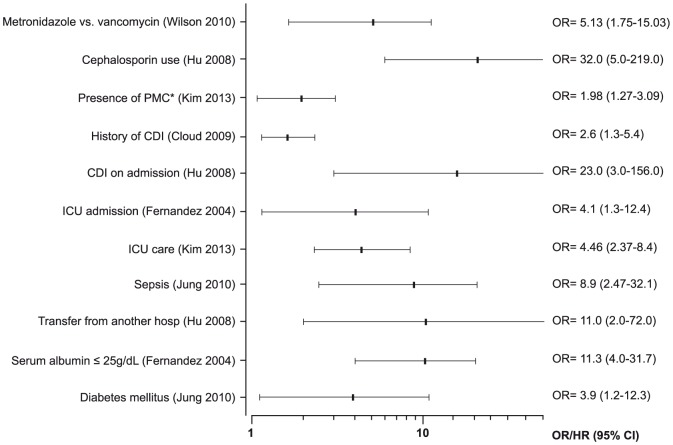
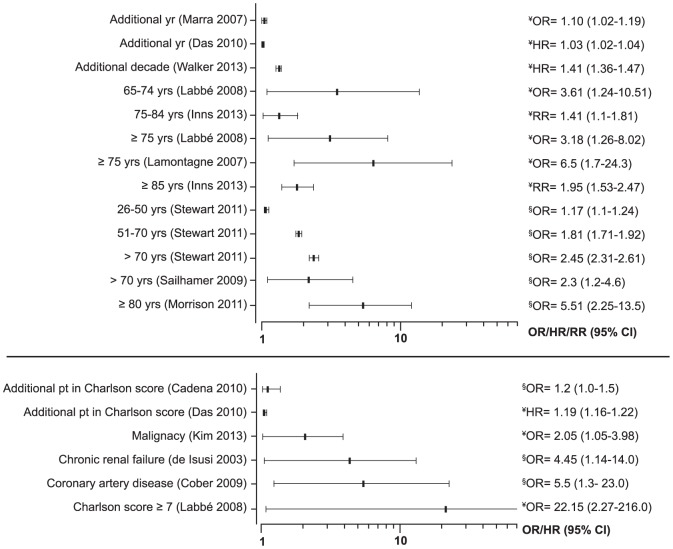
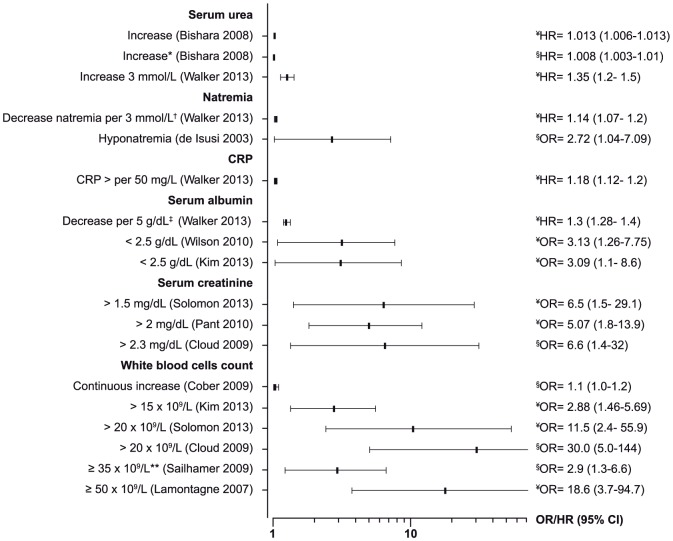
68 studies were included: 24 assessed risk factors for recurrence, 18 for complicated CDI, 8 for treatment failure, and 30 for mortality. Most studies accounted for mortality in the definition of complicated CDI. Important variables were inconsistently reported, such as previous episodes and use of antibiotics. Substantial heterogeneity and methodological limitations were noted, mainly in the sample size, the definition of the outcomes and periods of follow-up, precluding a meta-analysis. Older age, use of antibiotics after diagnosis, use of proton pump inhibitors, and strain type were the most frequent risk factors for recurrence. Older age, leucocytosis, renal failure and co-morbidities were frequent risk factors for complicated CDI. When considered alone, mortality was associated with age, co-morbidities, hypo-albuminemia, leucocytosis, acute renal failure, and infection with ribotype 027.
Laboratory parameters currently used in European and American guidelines to define patients at risk of a complicated CDI are adequate. Strategies for the management of CDI should be tailored according to the age of the patient, biological markers of severity, and underlying co-morbidities.
艰难梭菌感染(CDI)可导致并发症、复发和死亡。众多研究评估了这些不良结局的风险因素,但迄今为止发表的系统评价或荟萃分析在范围或质量上存在局限。
根据PRISMA指南完成了一项系统评价。在五个数据库中进行了电子检索。如果通过多变量分析评估了至少一种CDI结局的风险因素,则纳入截至2013年10月发表的研究。
纳入了68项研究:24项评估了复发的风险因素,18项评估了复杂性CDI的风险因素,8项评估了治疗失败的风险因素,30项评估了死亡率的风险因素。大多数研究在复杂性CDI的定义中考虑了死亡率。重要变量的报告不一致,如既往发作和抗生素的使用。注意到存在大量异质性和方法学局限性,主要体现在样本量、结局定义和随访期方面,因此无法进行荟萃分析。年龄较大、诊断后使用抗生素、使用质子泵抑制剂和菌株类型是复发最常见的风险因素。年龄较大、白细胞增多、肾衰竭和合并症是复杂性CDI常见的风险因素。单独考虑时,死亡率与年龄、合并症、低白蛋白血症、白细胞增多、急性肾衰竭以及027核糖体分型感染有关。
欧美指南中目前用于定义有复杂性CDI风险患者的实验室参数是足够的。CDI的管理策略应根据患者年龄、严重程度生物标志物和潜在合并症进行调整。