Viana Marina Verçoza, Moraes Rafael Barberena, Fabbrin Amanda Rodrigues, Santos Manoella Freitas, Torman Vanessa Bielefeldt Leotti, Vieira Silvia Regina, Gross Jorge Luiz, Canani Luis Henrique, Gerchman Fernando
Intensive Care Unit, Division of Endocrinology, Hospital de Clínicas de Porto Alegre, Federal University of Rio Grande do Sul, Porto Alegre, Brazil.
BMC Endocr Disord. 2014 Jun 17;14:50. doi: 10.1186/1472-6823-14-50.
Obesity and diabetes mellitus are well-defined risk factors for cardiovascular mortality. The impact of antecedent hyperglycemia and body size on mortality in critical ill patients in intensive care units (ICUs) may vary across their range of values. Therefore, we prospectively analyzed the relationship between in-hospital mortality and preexisting hyperglycemia and body size in critically ill ICU patients to understand how mortality varied among normal, overweight, and obese patients and those with low, intermediate, and high glycated hemoglobin (HbA1c) levels.
Medical history, weight, height, physiologic variables, and HbA1c were obtained during the first 24 h for patients who were consecutively admitted to the high complexity ICU of Hospital de Clínicas de Porto Alegre, Brazil, from April to August 2011. The relationships between mortality and obesity and antecedent hyperglycemia were prospectively analyzed by cubic spline analysis and a Cox proportional hazards model.
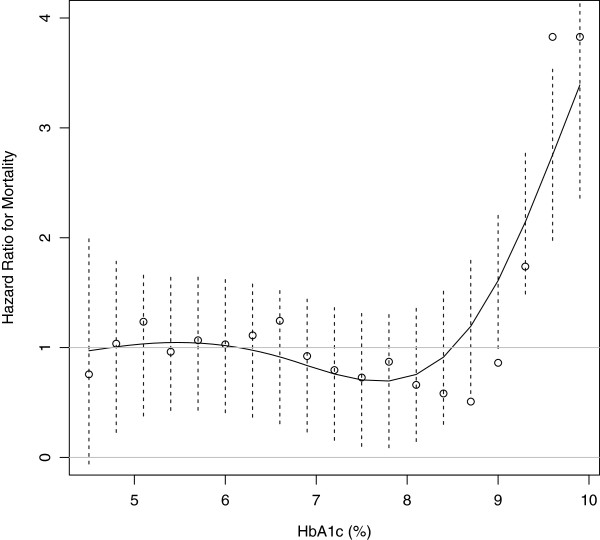
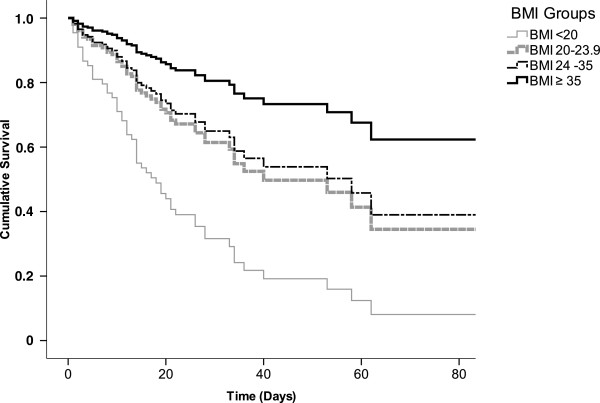
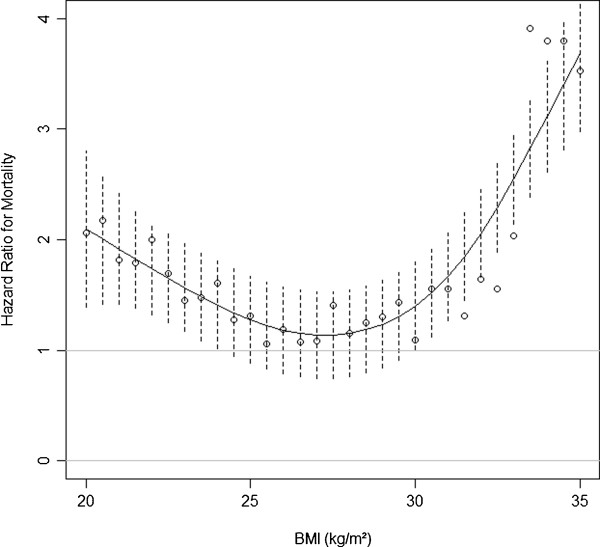
The study comprised 199 patients. The overall hospital mortality rate was 43.2% during a median 16 (8-28) days of follow-up. There was a progressive risk of in-hospital mortality with higher HbA1c levels, with the relationship becoming significant at HbA1c >9.3% compared with lower levels (hazard ratio 1.74; 95% confidence interval with Bonferroni correction 1.49-2.80). In contrast, mean body mass index (BMI) was higher in survivors than in nonsurvivors (27.2 kg/m2 ± 7.3 vs. 24.7 kg/m2 ± 5.0 P = 0.031, respectively). Cubic spline analysis showed that these relationships differed nonlinearly through the spectrum of BMI values. In a Cox proportional hazards model adjusted for Acute Physiology and Chronic Health Evaluation II score and HbA1c, the risk of in-hospital mortality progressively decreased with increasing BMI (BMI <20 vs. 20-23.9 kg/m2, P = 0.032; BMI <20 vs. 24-34.9 kg/m2, P = 0.010; BMI <20 vs. ≥35 kg/m2, P = 0.032).
Our findings suggest that significant hyperglycemia prior to ICU admission is a risk factor for in-hospital mortality. Conversely, increasing BMI may confer an advantageous effect against mortality in critical illness independently of previous glycemic control.
肥胖和糖尿病是心血管疾病死亡率明确的危险因素。在重症监护病房(ICU)中,先前存在的高血糖和体型对重症患者死亡率的影响可能因数值范围而异。因此,我们前瞻性地分析了重症ICU患者住院死亡率与先前存在的高血糖和体型之间的关系,以了解正常、超重和肥胖患者以及糖化血红蛋白(HbA1c)水平低、中、高的患者死亡率如何变化。
2011年4月至8月,连续入住巴西阿雷格里港临床医院高复杂性ICU的患者在入院后24小时内获取病史、体重、身高、生理变量和HbA1c。通过三次样条分析和Cox比例风险模型前瞻性分析死亡率与肥胖和先前高血糖之间的关系。
该研究包括199名患者。在中位随访16(8 - 28)天期间,总体医院死亡率为43.2%。随着HbA1c水平升高,住院死亡率风险逐渐增加,与较低水平相比,HbA1c>9.3%时这种关系变得显著(风险比1.74;经Bonferroni校正的95%置信区间为1.49 - 2.80)。相反,幸存者的平均体重指数(BMI)高于非幸存者(分别为27.2kg/m²±7.3和24.7kg/m²±5.0,P = 0.031)。三次样条分析表明,这些关系在BMI值范围内呈非线性差异。在根据急性生理与慢性健康状况评估II评分和HbA1c进行调整的Cox比例风险模型中,表示住院死亡率的风险随着BMI的增加而逐渐降低(BMI<20与20 - 23.9kg/m²相比,P = 0.032;BMI<20与24 - 34.9kg/m²相比,P = 0.010;BMI<20与≥35kg/m²相比,P = 0.032)。
我们的研究结果表明,ICU入院前显著的高血糖是住院死亡率的危险因素。相反,BMI增加可能独立于先前的血糖控制对重症患者的死亡率产生有利影响。