Centre for Health Economics, University of York, York, UK.
Australian Health Services Research Institute, University of Wollongong, Wollongong, Australia ; Department of Medical Statistics, Informatics and Health Economics, Innsbruck Medical University, Innsbruck, Austria.
Health Econ Rev. 2014 Apr 10;4:4. doi: 10.1186/s13561-014-0004-8. eCollection 2014.
The prospective reimbursement of hospitals through the grouping of patients into a finite number of categories (Diagnosis Related Groups, DRGs), is common to many European countries. However, the specific categories used vary greatly across countries, using different characteristics to define group boundaries and thus those characteristics which result in different payments for treatment. In order to assist in the construction and modification of national DRG systems, this study analyses the DRG systems of 10 European countries.
To compare the characteristics used to categorise patients receiving a coronary artery bypass graft (CABG) surgery into DRGs. Further, to compare the structure into which DRGs are placed and the relative price paid for patients across Europe.
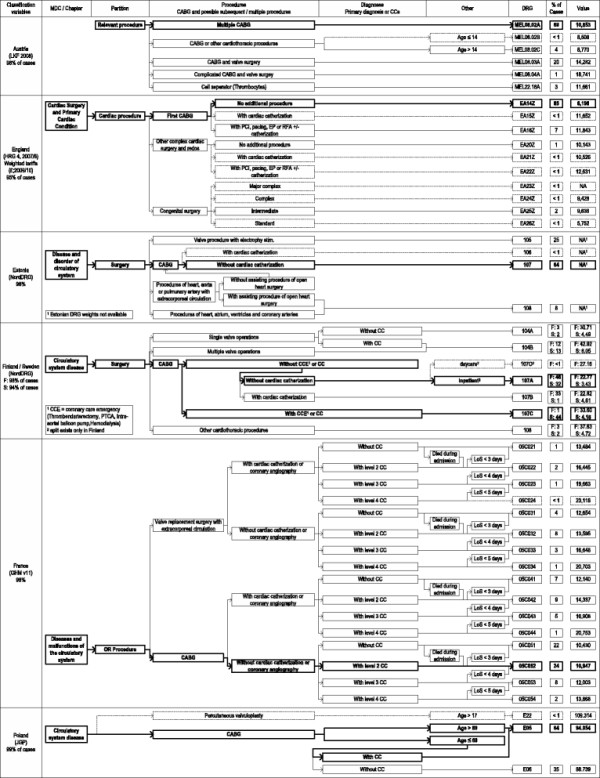
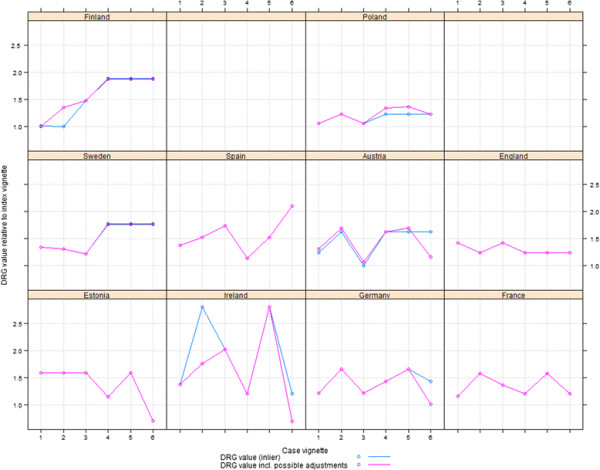
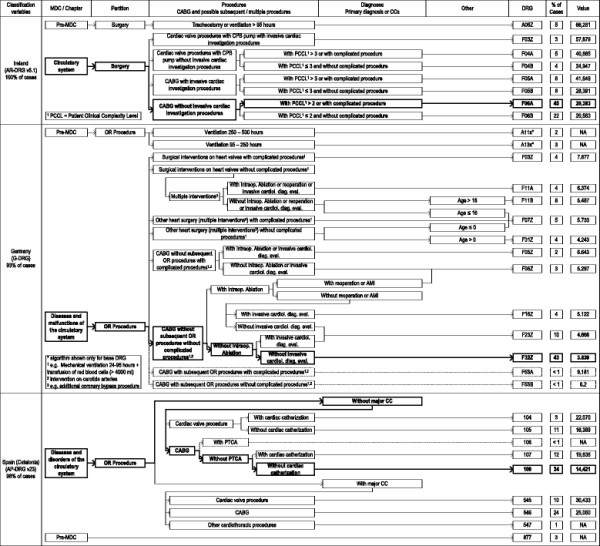
Patients with a procedure of CABG surgery are analysed from Austria, England, Estonia, Finland, France, Germany, Ireland, Poland, Spain and Sweden. Diagrammatic algorithms of DRG structures are presented for each country. The price in Euros of seven typical case vignettes, each made up of a set of a hypothetical patient's characteristics, is also analysed for each country. In order to enable comparisons across countries the simplest case (index vignette) is taken as baseline and relative price levels are calculated for the other six vignettes, each representing patients with different combinations of procedures and comorbidities.
European DRG payment structures for CABG surgery vary in terms of the number of different DRGs used and the types of distinctions which define patient categorisation. Based on the payments given to hospitals in different countries, the most resource intensive patient, relative to the index vignette, ranges in magnitude from 1.37 in Poland to 2.82 in Ireland. There is also considerable variation in how much different systems pay for particular circumstances, such as the occurrence of catheterisation or presence of comorbidity.
Past experience of the construction of DRG systems for CABG patients demonstrates the variety of options available. It also highlights the importance of updating systems as frequently as possible, to incentivise best practice.
通过将患者分为有限数量的类别(诊断相关组,DRGs)对医院进行前瞻性报销,在许多欧洲国家都很常见。然而,各国使用的具体类别差异很大,使用不同的特征来定义组边界,从而导致治疗费用的差异。为了协助构建和修改国家 DRG 系统,本研究分析了 10 个欧洲国家的 DRG 系统。
比较用于将接受冠状动脉旁路移植术(CABG)的患者分类为 DRGs 的特征。此外,比较欧洲各地放置 DRGs 的结构以及为患者支付的相对价格。
分析了来自奥地利、英国、爱沙尼亚、芬兰、法国、德国、爱尔兰、波兰、西班牙和瑞典的接受 CABG 手术的患者。为每个国家呈现了 DRG 结构的图表算法。还分析了每个国家七个典型病例的欧元价格,每个病例由一组假设患者特征组成。为了能够进行跨国比较,将最简单的病例(索引病例)作为基线,并为其他六个病例计算相对价格水平,每个病例代表不同手术和合并症组合的患者。
欧洲 CABG 手术的 DRG 支付结构在使用的不同 DRG 数量和定义患者分类的类型方面存在差异。基于不同国家医院收到的付款,相对于索引病例,资源最密集的患者的幅度从波兰的 1.37 到爱尔兰的 2.82。不同系统对特定情况(如导管插入术的发生或合并症的存在)的支付金额也存在很大差异。
过去构建 CABG 患者 DRG 系统的经验表明了可用选项的多样性。它还强调了尽可能频繁地更新系统的重要性,以激励最佳实践。