de Hoog Marieke L A, Venekamp Roderick P, van der Ent Cornelis K, Schilder Anne, Sanders Elisabeth Am, Damoiseaux Roger Amj, Bogaert Debby, Uiterwaal Cuno Spm, Smit Henriette A, Bruijning-Verhagen Patricia
Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, STR 6,131, PO Box 85500, 3508 GA Utrecht, The Netherlands.
BMC Med. 2014 Jun 26;12:107. doi: 10.1186/1741-7015-12-107.
Daycare attendance is an established risk factor for upper respiratory tract infections (URTI) and acute otitis media (AOM). Whether this results in higher use of healthcare resources during childhood remains unknown. We aim to assess the effect of first year daycare attendance on the timing and use of healthcare resources for URTI and AOM episodes during early childhood.
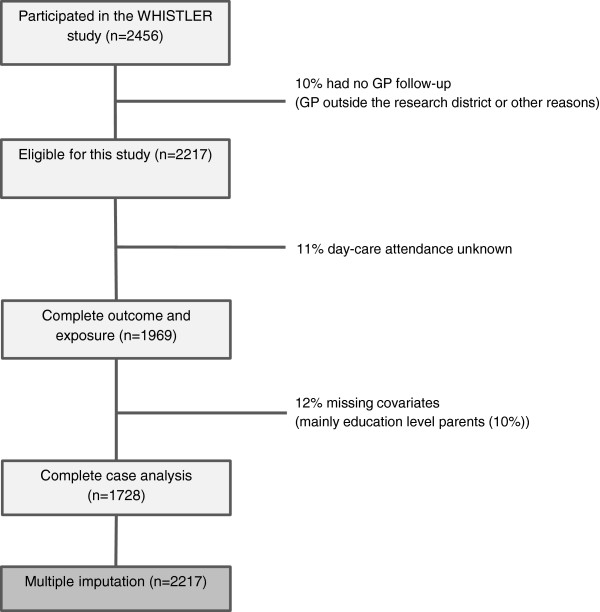
In the Wheezing-Illnesses-STudy-LEidsche-Rijn birth cohort, 2,217 children were prospectively followed up to age six years. Children were categorized according to first-year daycare attendance (yes versus no) and age at entry when applicable (age 0 to 2 months, 3 to 5 months and 6 to 12 months). Information on general practitioner (GP) diagnosed URTI and AOM, GP consultations, antibiotic prescriptions and specialist referral was collected from medical records. Daycare attendance was recorded by monthly questionnaires during the first year of life.
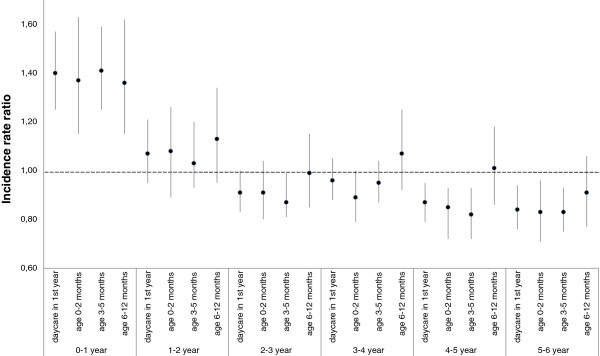
First-year daycare attendees and non-attendees had similar total six-year rates of GP-diagnosed URTI and AOM episodes (59/100 child-years, 95% confidence interval 57 to 61 versus 56/100 child-years, 53 to 59). Daycare attendees had more GP-diagnosed URTI and AOM episodes before the age of one year and fewer beyond the age of four years than non-attendees (Pinteraction <0.001). Daycare attendees had higher total six-year rates for GP consultation (adjusted rate ratio 1.15, 1.00 to 1.31) and higher risk for specialist referrals (hazard ratio: 1.43, 1.01 to 2.03). The number of antibiotic prescriptions in the first six years of life was only significantly increased among children who entered daycare between six to twelve months of age (rate ratio 1.32, 1.04 to 1.67). This subgroup of child-care attendees also had the highest overall URTI and AOM incidence rates, GP consultation rates and risk for specialist referral.
Children who enter daycare in the first year of life, have URTI and AOM at an earlier age, leading to higher use of healthcare resources compared to non-attendees, especially when entering daycare between six to twelve months. These findings emphasize the need for improved prevention strategies in daycare facilities to lower infection rates at the early ages.
日托是上呼吸道感染(URTI)和急性中耳炎(AOM)的既定风险因素。这是否会导致儿童时期医疗资源使用增加尚不清楚。我们旨在评估第一年日托对幼儿期URTI和AOM发作时医疗资源使用时间和使用情况的影响。
在莱顿莱茵河喘息疾病研究出生队列中,对2217名儿童进行了前瞻性随访至6岁。根据第一年是否参加日托(是与否)以及适用时的入园年龄(0至2个月、3至5个月和6至12个月)对儿童进行分类。从医疗记录中收集有关全科医生(GP)诊断的URTI和AOM、GP会诊、抗生素处方和专科转诊的信息。在生命的第一年通过每月问卷调查记录日托情况。
第一年参加日托的儿童和未参加日托的儿童在六年内被GP诊断为URTI和AOM发作的总发生率相似(59/100儿童年,95%置信区间57至61对56/100儿童年,53至59)。与未参加日托的儿童相比,参加日托的儿童在1岁之前被GP诊断为URTI和AOM发作的次数更多,在4岁之后更少(P交互作用<0.001)。参加日托的儿童六年内GP会诊的总发生率更高(调整率比1.15,1.00至1.31),专科转诊风险更高(风险比:1.43,1.01至2.03)。仅在六个月至十二个月大时进入日托的儿童在生命的前六年中抗生素处方数量显著增加(率比1.32,1.04至1.67)。这一日托儿童亚组的总体URTI和AOM发病率、GP会诊率和专科转诊风险也最高。
在生命第一年进入日托的儿童URTI和AOM发病年龄更早,与未参加日托的儿童相比,导致医疗资源使用增加,尤其是在六个月至十二个月大时进入日托。这些发现强调需要改进日托机构的预防策略以降低幼儿期感染率。