Klanova Magdalena, Lorkova Lucie, Vit Ondrej, Maswabi Bokang, Molinsky Jan, Pospisilova Jana, Vockova Petra, Mavis Cory, Lateckova Lucie, Kulvait Vojtech, Vejmelkova Dana, Jaksa Radek, Hernandez Francisco, Trneny Marek, Vokurka Martin, Petrak Jiri, Klener Pavel
Institute of Pathological Physiology, Charles University in Prague, First Faculty of Medicine, Prague, Czech Republic.
Mol Cancer. 2014 Jun 27;13:159. doi: 10.1186/1476-4598-13-159.
Mantle cell lymphoma (MCL) is an aggressive type of B-cell non-Hodgkin lymphoma associated with poor prognosis. Implementation of high-dose cytarabine (araC) into induction therapy became standard-of-care for all newly diagnosed younger MCL patients. However, many patients relapse even after araC-based regimen. Molecular mechanisms responsible for araC resistance in MCL are unknown and optimal treatment strategy for relapsed/refractory MCL patients remains elusive.
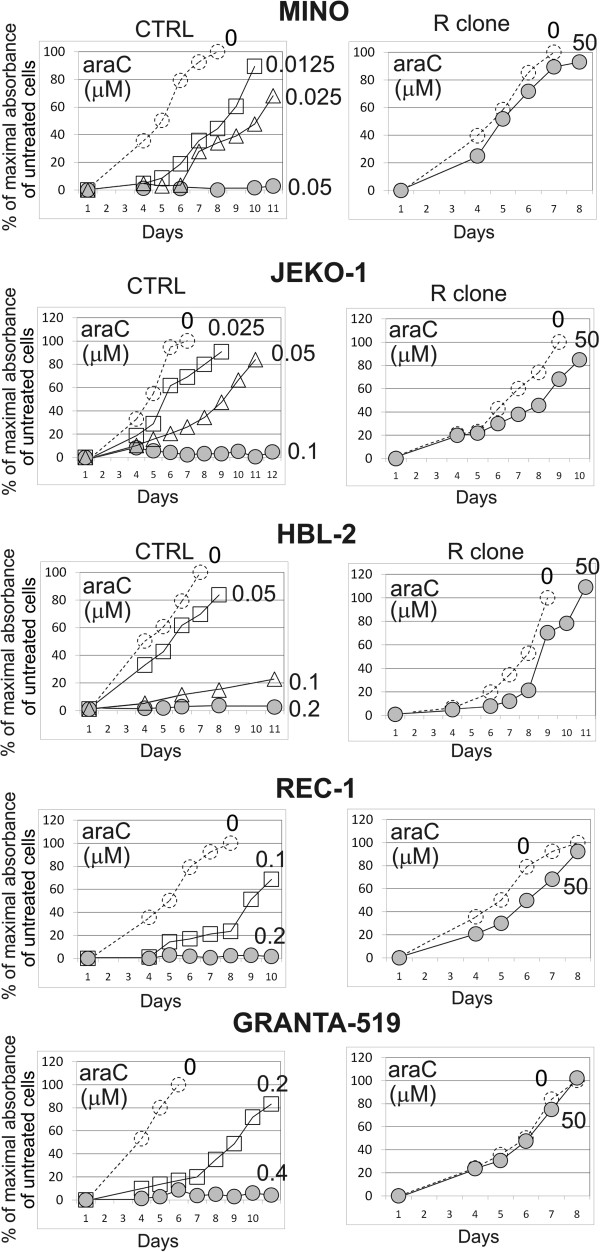
Five araC-resistant (R) clones were derived by long-term culture of five MCL cell lines (CTRL) with increasing doses of araC up to 50 microM. Illumina BeadChip and 2-DE proteomic analysis were used to identify gene and protein expression changes associated with araC resistance in MCL. In vitro cytotoxicity assays and experimental therapy of MCL xenografts in immunodeficient mice were used to analyze their relative responsiveness to a set of clinically used anti-MCL drugs. Primary MCL samples were obtained from patients at diagnosis and after failure of araC-based therapies.
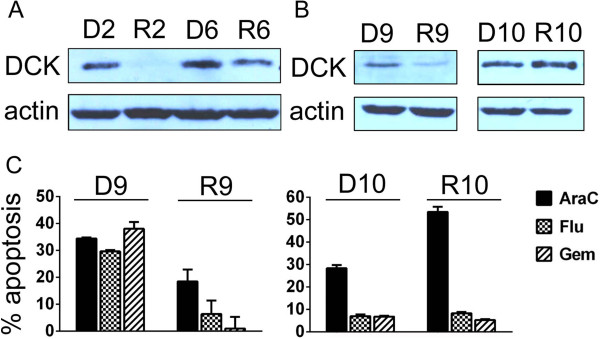
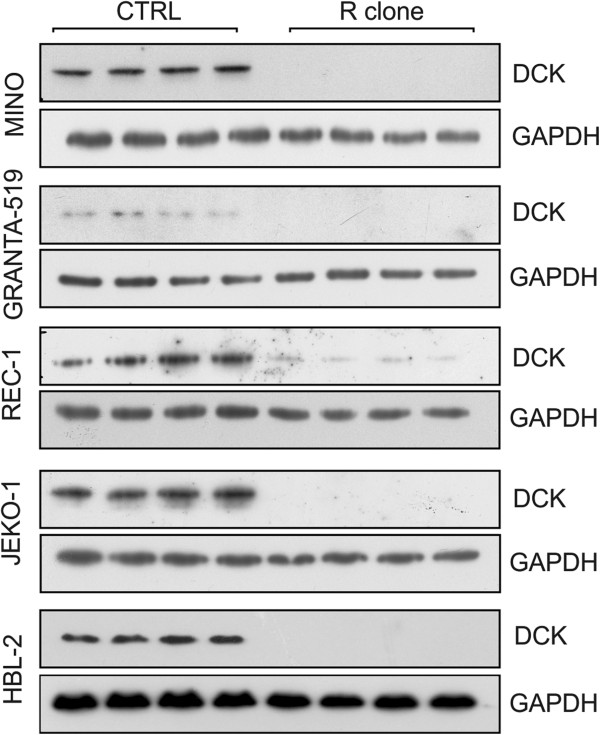
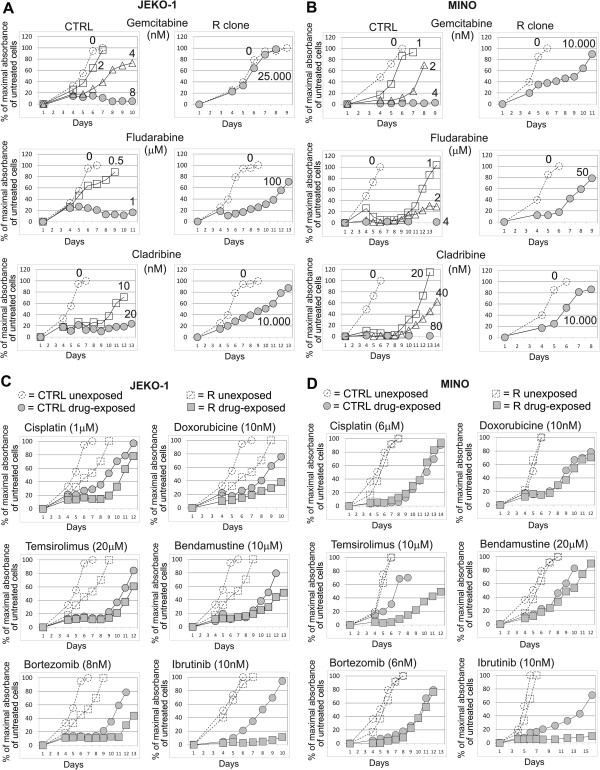
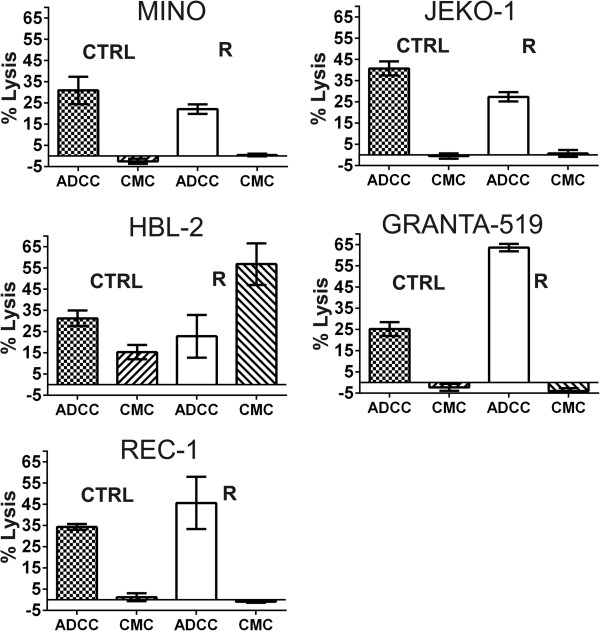
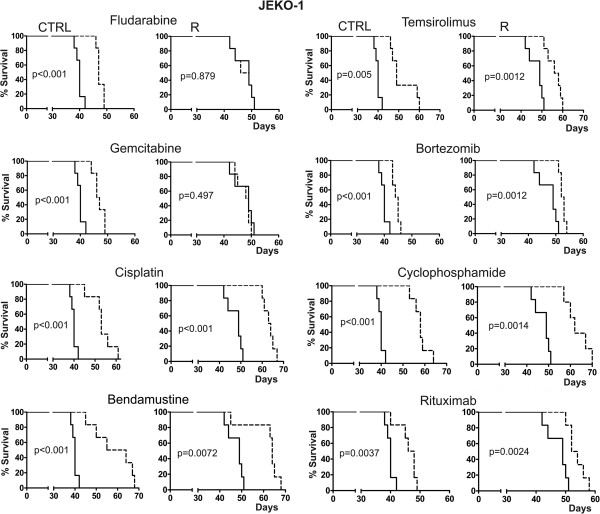
Marked downregulation of deoxycytidine-kinase (DCK) mRNA and protein expression was identified as the single most important molecular event associated with araC-resistance in all tested MCL cell lines and in 50% primary MCL samples. All R clones were highly (20-1000x) cross-resistant to all tested nucleoside analogs including gemcitabine, fludarabine and cladribine. In vitro sensitivity of R clones to other classes of clinically used anti-MCL agents including genotoxic drugs (cisplatin, doxorubicin, bendamustine) and targeted agents (bortezomib, temsirolimus, rituximab) remained unaffected, or was even increased (ibrutinib). Experimental therapy of immunodeficient mice confirmed the anticipated loss of anti-tumor activity (as determined by overall survival) of the nucleoside analogs gemcitabine and fludarabine in mice transplanted with R clone compared to mice transplanted with CTRL cells, while the anti-tumor activity of cisplatin, temsirolimus, bortezomib, bendamustine, cyclophosphamide and rituximab remained comparable between the two cohorts.
Acquired resistance of MCL cells to araC is associated with downregulation of DCK, enzyme of the nucleotide salvage pathway responsible for the first phosphorylation (=activation) of most nucleoside analogs used in anti-cancer therapy. The data suggest that nucleoside analogs should not be used in the therapy of MCL patients, who relapse after failure of araC-based therapies.
套细胞淋巴瘤(MCL)是一种侵袭性B细胞非霍奇金淋巴瘤,预后较差。在诱导治疗中采用大剂量阿糖胞苷(araC)已成为所有新诊断的年轻MCL患者的标准治疗方案。然而,许多患者即使在接受基于araC的方案治疗后仍会复发。MCL中导致araC耐药的分子机制尚不清楚,复发/难治性MCL患者的最佳治疗策略仍不明确。
通过对5种MCL细胞系(对照)进行长期培养,逐步增加araC剂量至50 microM,获得了5个araC耐药(R)克隆。使用Illumina BeadChip和二维蛋白质组分析来鉴定与MCL中araC耐药相关的基因和蛋白质表达变化。采用体外细胞毒性试验和免疫缺陷小鼠体内MCL异种移植实验疗法,分析它们对一组临床使用的抗MCL药物的相对反应性。原发性MCL样本取自诊断时及基于araC的治疗失败后的患者。
脱氧胞苷激酶(DCK)mRNA和蛋白质表达的显著下调被确定为所有测试的MCL细胞系以及50%的原发性MCL样本中与araC耐药相关的唯一最重要分子事件。所有R克隆对所有测试的核苷类似物包括吉西他滨、氟达拉滨和克拉屈滨均具有高度(20 - 1000倍)交叉耐药性。R克隆对其他临床使用的抗MCL药物类别包括基因毒性药物(顺铂、阿霉素、苯达莫司汀)和靶向药物(硼替佐米、替西罗莫司、利妥昔单抗)的体外敏感性未受影响,甚至有所增加(依鲁替尼)。免疫缺陷小鼠的实验疗法证实,与移植对照细胞的小鼠相比,移植R克隆的小鼠中核苷类似物吉西他滨和氟达拉滨的抗肿瘤活性(通过总生存期确定)预期丧失,而顺铂、替西罗莫司、硼替佐米、苯达莫司汀、环磷酰胺和利妥昔单抗在两个队列中的抗肿瘤活性相当。
MCL细胞对araC的获得性耐药与核苷酸补救途径中的酶DCK下调有关,该酶负责抗癌治疗中使用的大多数核苷类似物的首次磷酸化(=激活)。数据表明,对于基于araC的治疗失败后复发的MCL患者,不应使用核苷类似物进行治疗。