Department of Health Policy Planning and Management, Makerere University School of Public Health, PO Box 7072, Kampala, Uganda.
Department of International Health, Johns Hopkins Bloomberg School of Public Health, 615 North Wolfe Street, 21205 Baltimore, MD, USA.
Cost Eff Resour Alloc. 2014 Jun 19;12:14. doi: 10.1186/1478-7547-12-14. eCollection 2014.
High maternal and infant mortality continue to be major challenges to the attainment of the Millennium Development Goals for many low and middle-income countries. There is now evidence that voucher initiatives can increase access to maternal health services. However, a dearth of knowledge exists on the cost implications of voucher schemes. This paper estimates the incremental costs of a demand and supply side intervention aimed at increasing access to maternal health care services.
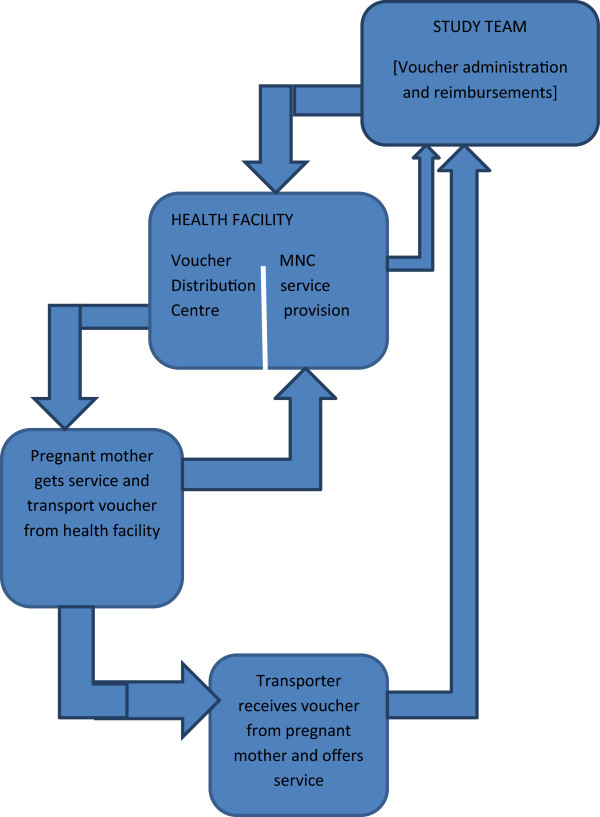
This costing study was part of a quasi-experimental voucher study conducted in two districts in Eastern Uganda to explore the impact of demand and supply - side incentives on increasing access to maternal health services. The provider's perspective was used and the ingredients approach to costing was employed. Costs were based on market prices as recorded in program records. Total, unit, and incremental costs were calculated.
The estimated total financial cost of the intervention for the one year of implementation was US$525,472 (US$1 = 2200UgShs). The major cost drivers included costs for transport vouchers (35.3%), health system strengthening (29.2%) and vouchers for maternal health services (18.2%). The average cost of transport per woman to and from the health facility was US$4.6. The total incremental costs incurred on deliveries (excluding caesarean section) was US$317,157 and US$107,890 for post natal care (PNC). The incremental costs per additional delivery and PNC attendance were US$23.9 and US$7.6 respectively.
Subsidizing maternal health care costs through demand and supply - side initiatives may not require significant amounts of resources contrary to what would be expected. With Uganda's Gross Domestic Product (GDP) per capita of US$55` (2012), the incremental cost per additional delivery (US$23.9) represents about 5% of GDP per capita to save a mother and probably her new born. For many low income countries, this may not be affordable, yet reliance on donor funding is often not sustainable. Alternative ways of raising additional resources for health must be explored. These include; encouraging private investments in critical sectors such as rural transport, health service provision; mobilizing households to save financial resources for preparedness, and financial targeting for the most vulnerable.
高孕产妇死亡率和婴儿死亡率仍然是许多中低收入国家实现千年发展目标的主要挑战。现在有证据表明,代金券计划可以增加获得产妇保健服务的机会。然而,对于代金券计划的成本影响,人们的了解还很匮乏。本文旨在评估一项旨在增加产妇保健服务可及性的供需方干预措施的增量成本。
本成本研究是在乌干达东部两个地区进行的准实验性代金券研究的一部分,旨在探索需求和供应方激励措施对增加产妇保健服务可及性的影响。本研究采用了提供者视角,并采用了成本核算成分法。成本基于方案记录中记录的市场价格。计算了总、单位和增量成本。
实施一年的干预措施的估计总财务成本为 525472 美元(1 美元=2200 乌干达先令)。主要成本驱动因素包括交通代金券(35.3%)、卫生系统加强(29.2%)和产妇保健服务代金券(18.2%)。每位妇女往返医疗机构的交通费用平均为 4.6 美元。分娩的总增量成本(不包括剖腹产)为 317157 美元,产后护理(PNC)的增量成本为 107890 美元。每增加一次分娩和 PNC 就诊的增量成本分别为 23.9 美元和 7.6 美元。
通过供需方举措补贴产妇保健费用可能不需要大量资源,这与人们的预期相反。按照乌干达 2012 年的人均国内生产总值(GDP)55 美元计算,每增加一次分娩的增量成本(23.9 美元)占人均 GDP 的 5%,可以拯救一位母亲,可能还有她的新生儿。对于许多低收入国家来说,这可能是负担不起的,但依赖捐助者资金往往是不可持续的。必须探索为卫生筹集额外资源的其他方法。这些方法包括:鼓励对农村交通、卫生服务提供等关键部门的私人投资;动员家庭为准备工作储蓄财政资源;以及对最弱势群体进行金融瞄准。