Cole Evan T, Harvey Greg, Urbanski Sara, Foster Gary, Thabane Lehana, Parker Melissa J
Department of Pediatrics, McMaster Children's Hospital and McMaster University, Hamilton, Ontario, Canada.
Department of Clinical Epidemiology and Biostatistics, McMaster University, Hamilton, Ontario, Canada Biostatistics Unit,/FSORC, St Joseph's Healthcare Hamilton, Hamilton, Canada.
BMJ Open. 2014 Jul 3;4(7):e005028. doi: 10.1136/bmjopen-2014-005028.
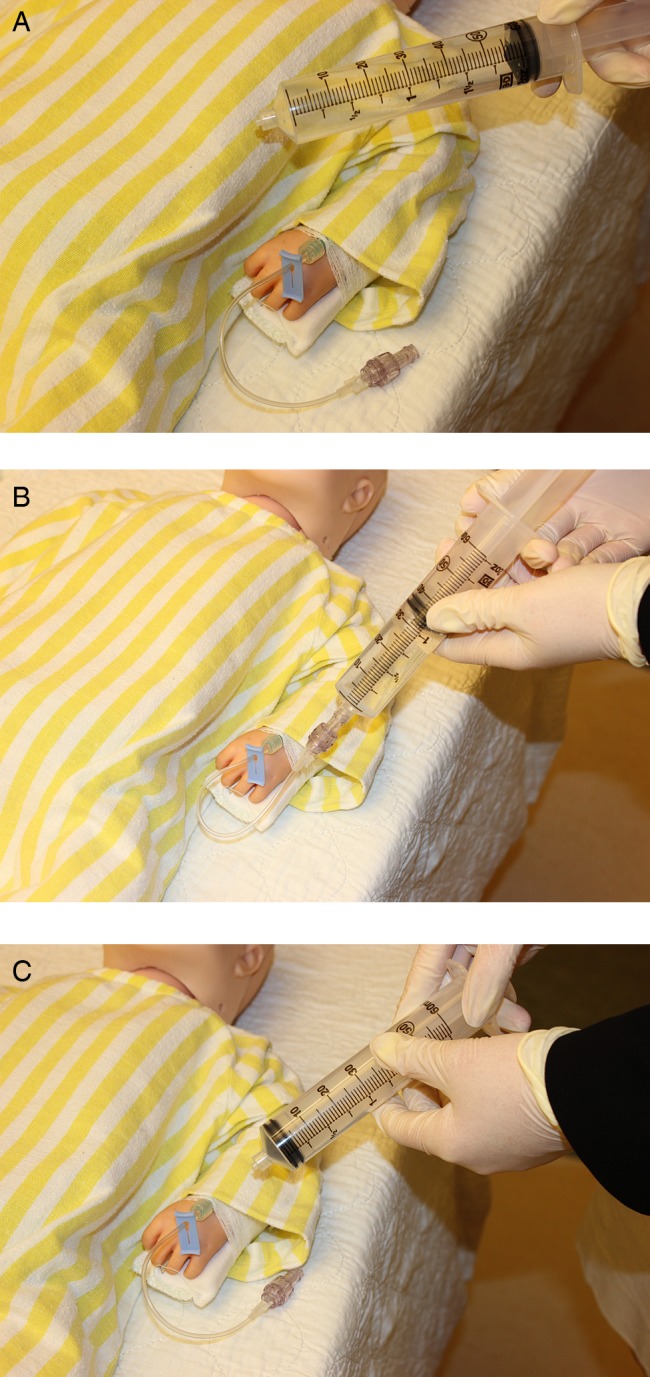
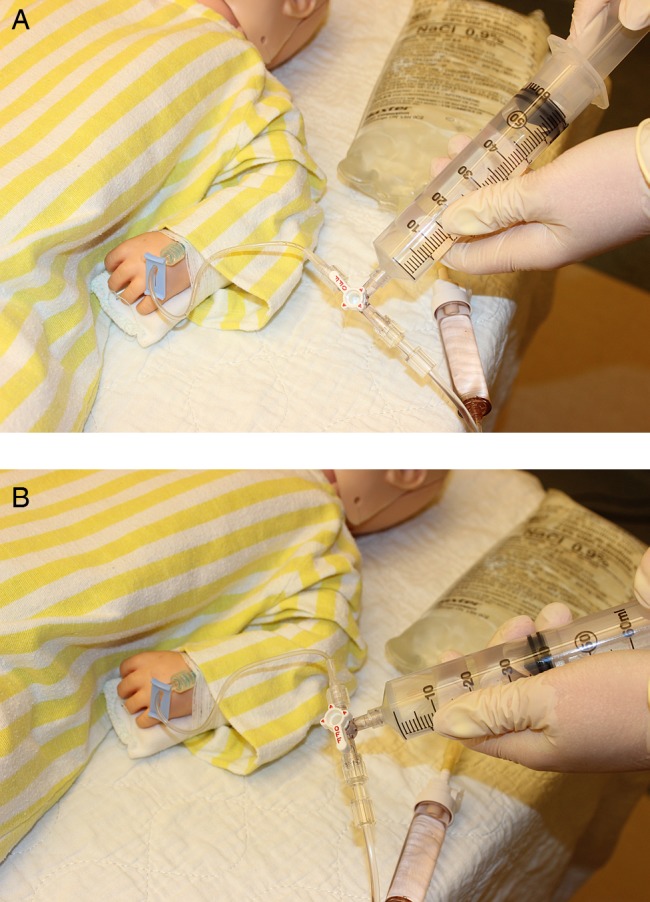
Manual techniques of intravascular fluid administration are commonly used during paediatric resuscitation, although it is unclear which technique is most efficient in the hands of typical healthcare providers. We compared the rate of fluid administration achieved with the disconnect-reconnect and push-pull manual syringe techniques for paediatric fluid resuscitation in a simulated setting.
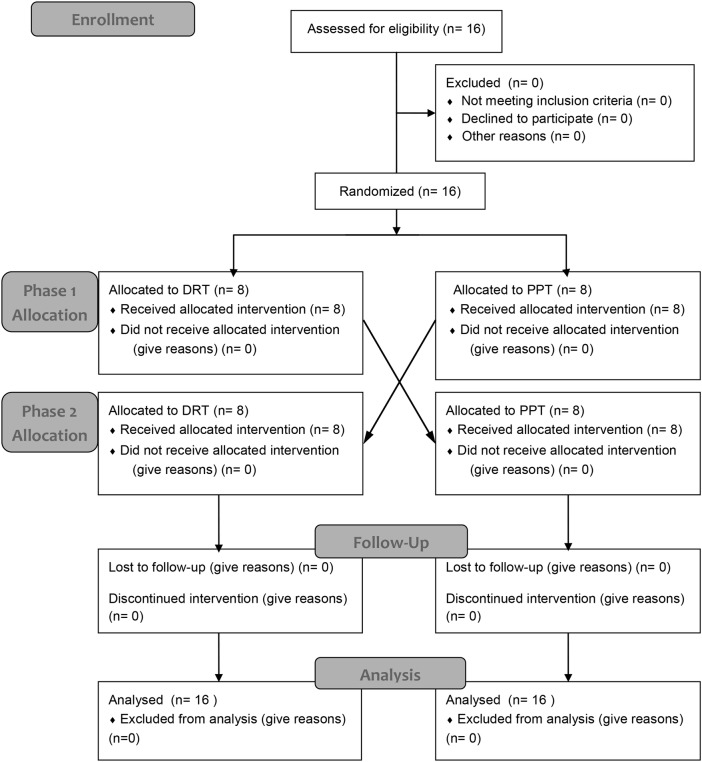
This study utilised a randomised crossover trial design and enrolled 16 consenting healthcare provider participants from a Canadian paediatric tertiary care centre. The study was conducted in a non-clinical setting using a model simulating a 15 kg child in decompensated shock. Participants administered 900 mL (60 mL/kg) of normal saline to the simulated patient using each of the two techniques under study. The primary outcome was the rate of fluid administration, as determined by two blinded independent video reviewers. We also collected participant demographic data and evaluated other secondary outcomes including total volume administered, number of catheter dislodgements, number of technical errors, and subjective and objective measures of provider fatigue.
All 16 participants completed the trial. The mean (SD) rate of fluid administration (mL/s) was greater for the disconnect-reconnect technique at 1.77 (0.145) than it was for the push-pull technique at 1.62 (0.226), with a mean difference of 0.15 (95% CI 0.055 to 0.251; p=0.005). There was no difference in mean volume administered (p=0.778) or participant self-reported fatigue (p=0.736) between techniques. No catheter dislodgement events occurred.
The disconnect-reconnect technique allowed for the fastest rate of fluid administration, suggesting that use of this technique may be preferable in situations requiring rapid resuscitation. These findings may help to inform future iterations of paediatric resuscitation guidelines.
This trial was registered at ClinicalTrials.gov [NCT01774214] prior to enrolling the first participant.
在儿科复苏过程中,血管内液体输注的手动技术被广泛应用,然而尚不清楚在普通医护人员手中哪种技术效率最高。我们在模拟环境中比较了用于儿科液体复苏的断开 - 重新连接和推拉式手动注射器技术的液体输注速率。
本研究采用随机交叉试验设计,招募了来自加拿大一家儿科三级护理中心的16名同意参与的医护人员。研究在非临床环境中进行,使用模拟一名15公斤失代偿性休克儿童的模型。参与者使用所研究的两种技术中的每一种,向模拟患者输注900毫升(60毫升/公斤)生理盐水。主要结局是液体输注速率,由两名 blinded 独立视频评审员确定。我们还收集了参与者的人口统计学数据,并评估了其他次要结局,包括输注的总体积、导管移位次数、技术错误次数以及医护人员疲劳的主观和客观指标。
所有16名参与者均完成试验。断开 - 重新连接技术的平均(标准差)液体输注速率(毫升/秒)为1.77(0.145),高于推拉式技术的1.62(0.226),平均差值为0.15(95%可信区间0.055至0.251;p = 0.005)。两种技术在平均输注体积(p = 0.778)或参与者自我报告的疲劳程度(p = 0.736)方面没有差异。未发生导管移位事件。
断开 -重新连接技术实现了最快的液体输注速率,这表明在需要快速复苏的情况下使用该技术可能更可取。这些发现可能有助于为未来儿科复苏指南的修订提供参考。
本试验在招募第一名参与者之前已在ClinicalTrials.gov [NCT01774214] 注册。