Abraham Mary B, Rao Shripada, Price Glynis, Choong Catherine S
Department of Endocrinology and Diabetes, Princess Margaret Hospital, Perth, Australia.
Department of Neonatology, Princess Margaret Hospital, Perth, Australia.
Int J Pediatr Endocrinol. 2014;2014(1):11. doi: 10.1186/1687-9856-2014-11. Epub 2014 Jun 20.
The treatment of central diabetes insipidus (DI) with desmopressin in the neonatal period is challenging because of the significant risk of hyponatremia with this agent. The fixed anti-diuresis action of desmopressin and the obligate high fluid intake with milk feeds lead to considerable risk of water intoxication and hyponatremia. To reduce this risk, thiazide diuretics, part of the treatment of nephrogenic DI, were used in conjunction with low renal solute feed and were effective in a single case series of neonatal central DI.
We evaluated the efficacy of early treatment of neonatal central DI with hydrochlorothiazide with low solute feed and investigated the clinical indicators for transition to desmopressin during infancy.
A retrospective chart review was conducted at Princess Margaret Hospital, Perth of neonates diagnosed with central DI and treated with hydrochlorothiazide, between 2007 and 2013. Four newborns were identified. Mean sNa and mean change in sNa with desmopressin and hydrochlorothiazide treatment were recorded along with episodes of hyponatremia and hypernatremia. Length and weight trajectories during the first 12 months were assessed.
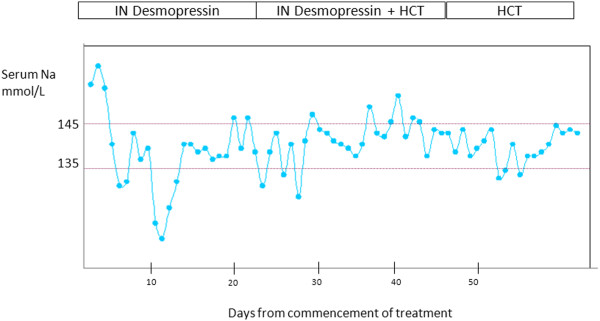
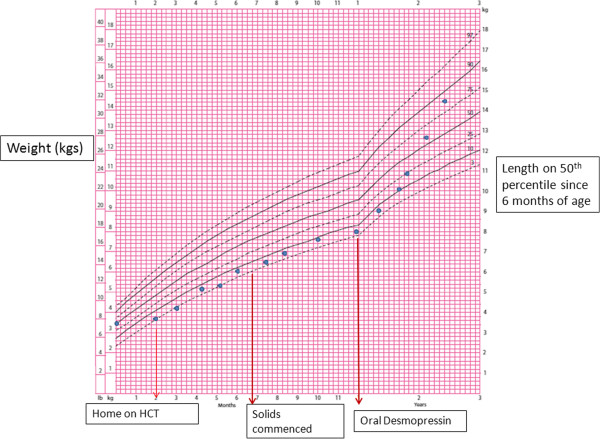
The mean change in sNa per day with hydrochlorothiazide and low renal solute feed was 2.5 - 3 mmol/L; on desmopressin treatment, the mean change in sNa was 6.8-7.9 mmol/L. There was one episode of symptomatic hyponatremia with intranasal desmopressin with no episodes of hyponatremia or hypernatremia during treatment with hydrochlorothiazide or following transition to oral desmopressin. Transition to oral desmopressin between 3 to 12 months of age was associated with good control of DI. Following introduction of solids, sNa remained stable but weight gain was slow. This improved following transition to desmopressin in one infant.
Hydrochlorothiazide with low renal solute feed is a safe and effective treatment option in neonatal central DI. However, transition to desmopressin should be considered early in infancy following initiation of solids to facilitate growth.
在新生儿期使用去氨加压素治疗中枢性尿崩症(DI)具有挑战性,因为使用该药物存在显著的低钠血症风险。去氨加压素固定的抗利尿作用以及因喂奶而必须大量摄入液体,导致水中毒和低钠血症的风险相当高。为降低此风险,噻嗪类利尿剂(用于治疗肾性尿崩症的一部分)与低肾溶质喂养联合使用,并在一个新生儿中枢性尿崩症的单病例系列中取得了成效。
我们评估了早期使用氢氯噻嗪联合低溶质喂养治疗新生儿中枢性尿崩症的疗效,并研究了婴儿期过渡到使用去氨加压素的临床指标。
对2007年至2013年期间在珀斯玛格丽特公主医院被诊断为中枢性尿崩症并接受氢氯噻嗪治疗的新生儿进行回顾性病历审查。共确定了4名新生儿。记录了使用去氨加压素和氢氯噻嗪治疗期间的平均血清钠(sNa)以及sNa的平均变化,同时记录低钠血症和高钠血症发作情况。评估了前12个月的身长和体重轨迹。
氢氯噻嗪联合低肾溶质喂养时,sNa每天的平均变化为2.5 - 3 mmol/L;使用去氨加压素治疗时,sNa的平均变化为6.8 - 7.9 mmol/L。使用鼻内去氨加压素时有1次症状性低钠血症发作,而在使用氢氯噻嗪治疗期间或过渡到口服去氨加压素后,无低钠血症或高钠血症发作。3至12个月龄时过渡到口服去氨加压素与尿崩症得到良好控制相关。引入固体食物后,sNa保持稳定,但体重增加缓慢。1名婴儿过渡到使用去氨加压素后情况有所改善。
氢氯噻嗪联合低肾溶质喂养是新生儿中枢性尿崩症的一种安全有效的治疗选择。然而,在开始添加固体食物后应尽早考虑过渡到使用去氨加压素,以促进生长。