Bigogo Godfrey, Amolloh Manase, Laserson Kayla F, Audi Allan, Aura Barrack, Dalal Warren, Ackers Marta, Burton Deron, Breiman Robert F, Feikin Daniel R
Center for Global Health Research, Kenya Medical Research Institute, P,O, Box 1578, 40100 Kisumu, Kenya.
BMC Infect Dis. 2014 Jul 8;14:376. doi: 10.1186/1471-2334-14-376.
In much of Africa, most individuals living with HIV do not know their status. Home-based counseling and testing (HBCT) leads to more HIV-infected people learning their HIV status. However, there is little data on whether knowing one's HIV-positive status necessarily leads to uptake of HIV care, which could in turn, lead to a reduction in the prevalence of common infectious disease syndromes.
In 2008, Kenya Medical Research Institute (KEMRI) in collaboration with the Centers for Disease Control and Prevention (CDC) offered HBCT to individuals (aged ≥13 years) under active surveillance for infectious disease syndromes in Lwak in rural western Kenya. HIV test results were linked to morbidity and healthcare-seeking data collected by field workers through bi-weekly home visits. We analyzed changes in healthcare seeking behaviors using proportions, and incidence (expressed as episodes per person-year) of acute respiratory illness (ARI), severe acute respiratory illness (SARI), acute febrile illness (AFI) and diarrhea among first-time HIV testers in the year before and after HBCT, stratified by their test result and if HIV-positive, whether they sought care at HIV Patient Support Centers (PSCs).
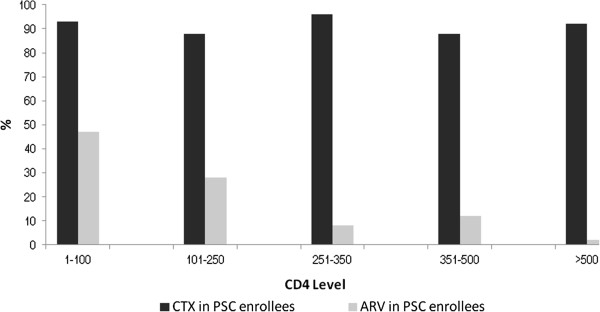
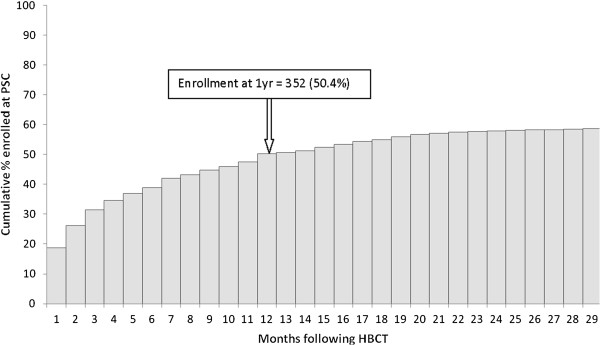
Of 9,613 individuals offered HBCT, 6,366 (66%) were first-time testers, 698 (11%) of whom were HIV-infected. One year after HBCT, 50% of HIV-infected persons had enrolled at PSCs - 92% of whom had started cotrimoxazole and 37% of those eligible for antiretroviral treatment had initiated therapy. Among HIV-infected persons enrolled in PSCs, AFI and diarrhea incidence decreased in the year after HBCT (rate ratio [RR] 0.84; 95% confidence interval [CI] 0.77 - 0.91 and RR 0.84, 95% CI 0.73 - 0.98, respectively). Among HIV-infected persons not attending PSCs and among HIV-uninfected persons, decreases in incidence were significantly lower. While decreases also occurred in rates of respiratory illnesses among HIV-positive persons in care, there were similar decreases in the other two groups.
Large scale HBCT enabled a large number of newly diagnosed HIV-infected persons to know their HIV status, leading to a change in care seeking behavior and ultimately a decrease in incidence of common infectious disease syndromes through appropriate treatment and care.
在非洲大部分地区,大多数艾滋病毒感染者并不知道自己的感染状况。居家咨询与检测(HBCT)使更多艾滋病毒感染者了解了自己的感染状况。然而,关于知晓自己的艾滋病毒阳性状况是否必然会促使其接受艾滋病毒治疗的数据很少,而接受治疗反过来可能会降低常见传染病综合征的患病率。
2008年,肯尼亚医学研究所(KEMRI)与美国疾病控制与预防中心(CDC)合作,为肯尼亚西部农村地区卢瓦克正在接受传染病综合征主动监测的13岁及以上个人提供居家咨询与检测服务。艾滋病毒检测结果与现场工作人员通过每两周一次的家访收集的发病率和就医数据相关联。我们使用比例分析了就医行为的变化,以及居家咨询与检测前后首次接受艾滋病毒检测者中急性呼吸道疾病(ARI)、严重急性呼吸道疾病(SARI)、急性发热性疾病(AFI)和腹泻的发病率(以每人每年发病次数表示),并按检测结果分层,对于艾滋病毒呈阳性者,还按其是否在艾滋病毒患者支持中心(PSC)寻求治疗进行分层。
在9613名接受居家咨询与检测的个人中,6366人(66%)是首次检测者,其中698人(11%)感染了艾滋病毒。居家咨询与检测一年后,50%的艾滋病毒感染者已在患者支持中心登记——其中92%已开始服用复方新诺明,符合抗逆转录病毒治疗条件的感染者中有37%已开始接受治疗。在登记到患者支持中心的艾滋病毒感染者中,居家咨询与检测后的那一年,急性发热性疾病和腹泻的发病率有所下降(率比[RR]分别为0.84;95%置信区间[CI]为0.77 - 0.91和RR 0.84,95% CI为0.73 - 0.98)。在未到患者支持中心就诊的艾滋病毒感染者以及未感染艾滋病毒的人群中,发病率的下降幅度明显较小。虽然接受治疗的艾滋病毒阳性者的呼吸道疾病发病率也有所下降,但其他两组也有类似程度的下降。
大规模的居家咨询与检测使大量新诊断出的艾滋病毒感染者了解了自己的感染状况,导致就医行为发生改变,并最终通过适当的治疗和护理降低了常见传染病综合征的发病率。