Bozkurt Ahmet, van Neerven Sabien G A, Claeys Kristl G, O'Dey Dan Mon, Sudhoff Angela, Brook Gary A, Sellhaus Bernd, Schulz Jörg B, Weis Joachim, Pallua Norbert
Department of Plastic Surgery, Reconstructive and Hand Surgery, Burn Centre, Medical Faculty, RWTH Aachen University Hospital, Pauwelsstraße 30, 52074 Aachen, Germany.
Department of Neurology, Medical Faculty, RWTH Aachen University, 52074 Aachen, Germany ; Institute of Neuropathology, RWTH Aachen University Hospital, 52074 Aachen, Germany ; JARA, Translational Brain Medicine, 52074 Aachen, Germany.
Biomed Res Int. 2014;2014:121452. doi: 10.1155/2014/121452. Epub 2014 Jun 2.
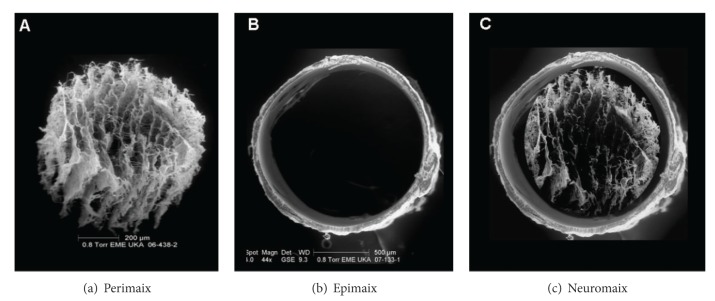
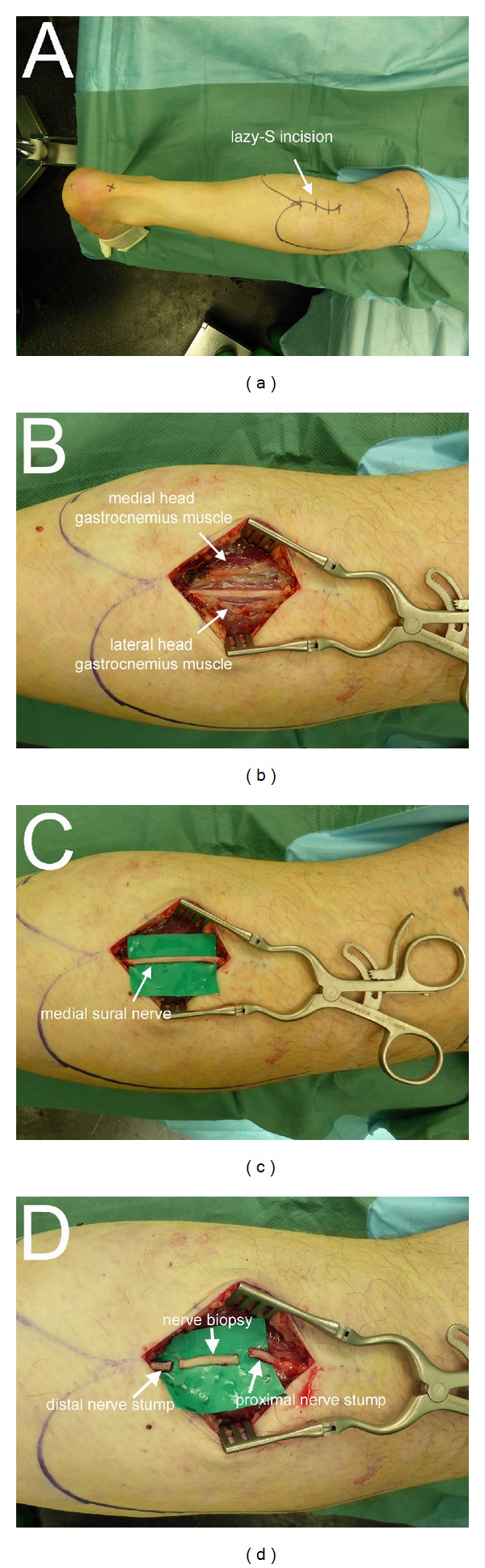
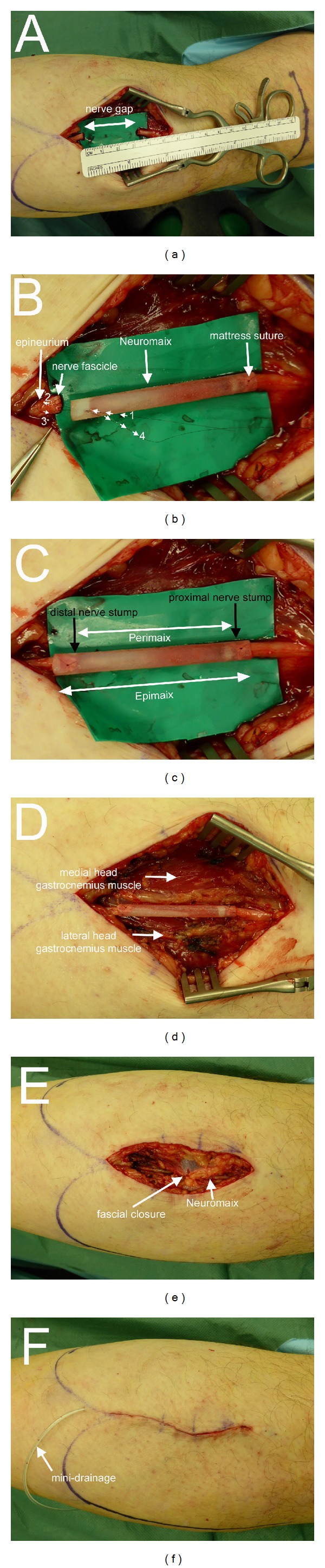
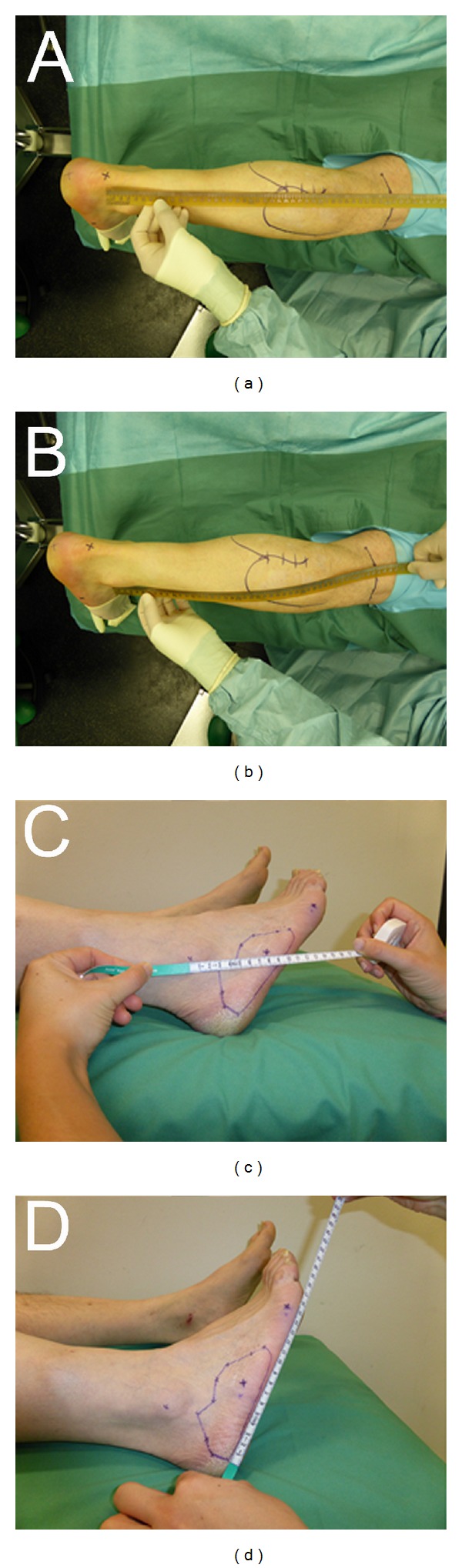
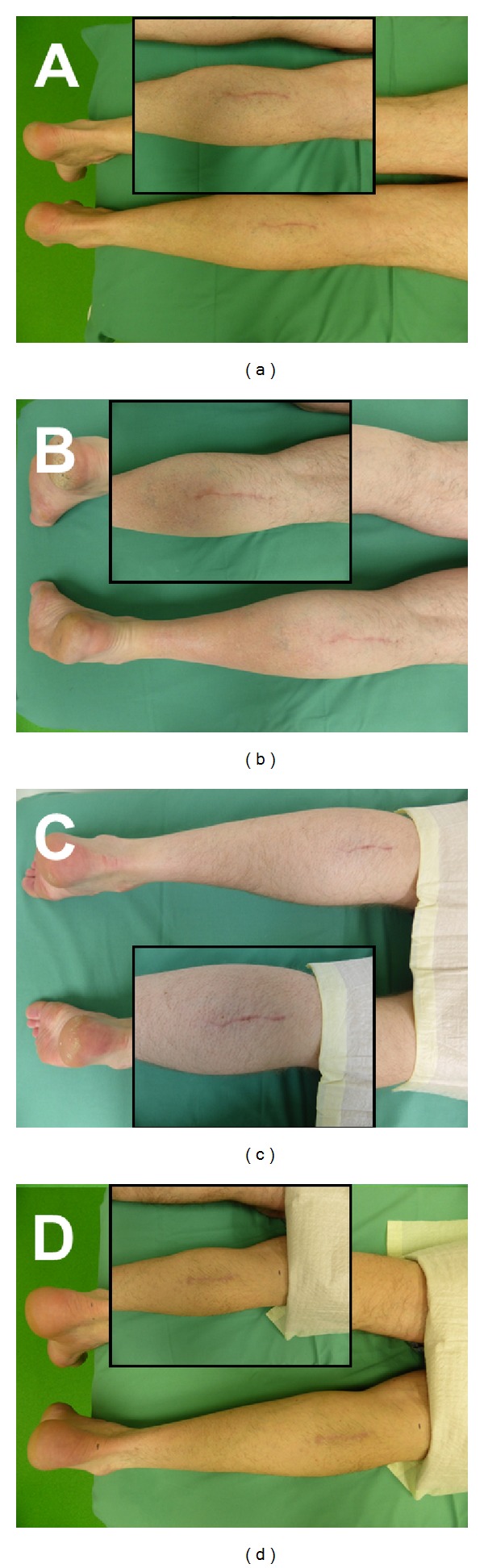
Autologous nerve transplantation (ANT) is the clinical gold standard for the reconstruction of peripheral nerve defects. A large number of bioengineered nerve guides have been tested under laboratory conditions as an alternative to the ANT. The step from experimental studies to the implementation of the device in the clinical setting is often substantial and the outcome is unpredictable. This is mainly linked to the heterogeneity of clinical peripheral nerve injuries, which is very different from standardized animal studies. In search of a reproducible human model for the implantation of bioengineered nerve guides, we propose the reconstruction of sural nerve defects after routine nerve biopsy as a first or baseline study. Our concept uses the medial sural nerve of patients undergoing diagnostic nerve biopsy (≥ 2 cm). The biopsy-induced nerve gap was immediately reconstructed by implantation of the novel microstructured nerve guide, Neuromaix, as part of an ongoing first-in-human study. Here we present (i) a detailed list of inclusion and exclusion criteria, (ii) a detailed description of the surgical procedure, and (iii) a follow-up concept with multimodal sensory evaluation techniques. The proximal medial sural nerve biopsy model can serve as a preliminary nature of the injuries or baseline nerve lesion model. In a subsequent step, newly developed nerve guides could be tested in more unpredictable and challenging clinical peripheral nerve lesions (e.g., following trauma) which have reduced comparability due to the different nature of the injuries (e.g., site of injury and length of nerve gap).
自体神经移植(ANT)是周围神经缺损重建的临床金标准。大量生物工程神经导管已在实验室条件下作为ANT的替代方案进行了测试。从实验研究到该装置在临床环境中的应用这一步往往很大,且结果不可预测。这主要与临床周围神经损伤的异质性有关,这与标准化动物研究有很大不同。为了寻找一种可重复的用于植入生物工程神经导管的人体模型,我们提议将常规神经活检后的腓肠神经缺损重建作为一项初步或基线研究。我们的概念使用接受诊断性神经活检(≥2 cm)患者的腓肠内侧神经。作为正在进行的首次人体研究的一部分,通过植入新型微结构神经导管Neuromaix立即重建活检引起的神经间隙。在此,我们展示(i)详细的纳入和排除标准列表,(ii)手术过程的详细描述,以及(iii)采用多模态感觉评估技术的随访概念。近端腓肠内侧神经活检模型可作为损伤的初步性质或基线神经损伤模型。在后续步骤中,可以在更不可预测且具有挑战性的临床周围神经损伤(例如创伤后)中测试新开发的神经导管,这些损伤由于损伤性质不同(例如损伤部位和神经间隙长度)而可比性降低。