Han Weiyu, Cai Shiji, Liu Zhenhua, Jin Xingzhong, Wang Xia, Antony Benny, Cao Yuelong, Aitken Dawn, Cicuttini Flavia, Jones Graeme, Ding Changhai
Arthritis Res Ther. 2014 Jul 9;16(4):R145. doi: 10.1186/ar4607.
Recent studies regarding the infrapatellar fat pad (IPFP) mainly focus on the roles of the cells derived from the IPFP. There have been few clinical or epidemiological studies reporting on the association between the IPFP and knee osteoarthritis (OA). Our objective is to generate hypotheses regarding the associations between IPFP maximum area and knee OA measures in older adults.
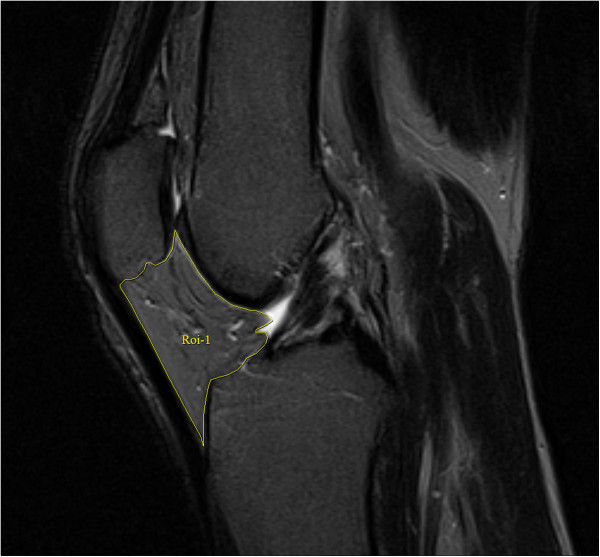
A total of 977 subjects between 50 and 80 years of age (mean, 62.4 years) participated in the study. Radiographic knee osteophyte and joint space narrowing (JSN) were assessed using the Osteoarthritis Research Society International atlas. T1- or T2-weighted fat suppressed magnetic resonance imaging (MRI) was utilized to assess IPFP maximum area, cartilage volume, cartilage defects, and bone marrow lesions (BMLs). Knee pain was assessed by self-administered Western Ontario McMaster Osteoarthritis Index (WOMAC) questionnaire.
After adjustment for potential confounders, IPFP maximum area was significantly associated with joint space narrowing (odds ratio (OR): 0.75, 95% confidence interval (CI): 0.62 to 0.91 (medial), 0.77, 95% CI: 0.62 to 0.96 (lateral)) and medial osteophytes (OR: 0.52, 95% CI: 0.35 to 0.76), knee tibial and patellar cartilage volume (β: 56.9 to 164.9 mm3/cm2, all P <0.001), tibial cartilage defects (OR: 0.58, 95% CI: 0.41 to 0.81 (medial), 0.53, 95% CI: 0.40-0.71 (lateral)), any BMLs (OR: 0.77, 95% CI: 0.63 to 0.94), and knee pain on a flat surface (OR: 0.79, 95% CI: 0.63 to 0.98). IPFP maximum area was negatively, but not significantly, associated with femoral cartilage defects, lateral tibiofemoral BMLs, and total knee pain or other knee pain subscales.
IPFP maximum area is beneficially associated with radiographic OA, MRI structural pathology and knee pain on a flat surface suggesting a protective role for IPFP possibly through shock absorption. Consequently, we must pay special attention to IPFP in the clinical settings, avoiding resection of normal IPFP in knee surgery.
近期关于髌下脂肪垫(IPFP)的研究主要集中在源自IPFP的细胞的作用上。很少有临床或流行病学研究报道IPFP与膝关节骨关节炎(OA)之间的关联。我们的目的是提出关于老年人IPFP最大面积与膝关节OA指标之间关联的假设。
共有977名年龄在50至80岁(平均62.4岁)之间的受试者参与了该研究。使用国际骨关节炎研究学会图谱评估膝关节X线骨赘和关节间隙变窄(JSN)。利用T1加权或T2加权脂肪抑制磁共振成像(MRI)评估IPFP最大面积、软骨体积、软骨缺损和骨髓病变(BMLs)。通过自我填写的西安大略和麦克马斯特大学骨关节炎指数(WOMAC)问卷评估膝关节疼痛。
在对潜在混杂因素进行调整后,IPFP最大面积与关节间隙变窄(优势比(OR):0.75,95%置信区间(CI):0.62至0.91(内侧),0.77,95%CI:0.62至0.96(外侧))和内侧骨赘(OR:0.52,95%CI:0.35至0.76)、膝关节胫骨和髌骨软骨体积(β:56.9至164.9mm³/cm²,所有P<0.001)、胫骨软骨缺损(OR:0.58,95%CI:0.41至0.81(内侧),0.53,95%CI:0.40 - 0.71(外侧))、任何BMLs(OR:0.77,95%CI:0.63至0.94)以及平地上的膝关节疼痛(OR:0.79,95%CI:0.63至0.98)显著相关。IPFP最大面积与股骨软骨缺损、外侧胫股关节BMLs以及全膝关节疼痛或其他膝关节疼痛亚量表呈负相关,但无显著意义。
IPFP最大面积与X线OA、MRI结构病理学以及平地上的膝关节疼痛呈有益关联,提示IPFP可能通过减震起到保护作用。因此,我们在临床环境中必须特别关注IPFP,在膝关节手术中避免切除正常的IPFP。