Kjelstrup Trygve, Hol Per K, Courivaud Frédéric, Smith Hans-Jørgen, Røkkum Magne, Klaastad Øivind
From the Department of Anaesthesiology, Diakonhjemmet Hospital (TK), The Intervention Centre, Oslo University Hospital, Rikshospitalet, Oslo (TK, PKH, FC), Department of Radiology and Nuclear Medicine, Oslo University Hospital, Oslo (HJS), Department of Orthopaedics, Oslo University Hospital, Rikshospitalet, Oslo (MR), Department of Anaesthesiology, University Hospital of North Norway and Institute of Clinical Medicine, University of Tromsø, Tromsø (ØK) and Institute of Clinical Medicine, University of Oslo, Oslo, Norway (HJS, MR).
Eur J Anaesthesiol. 2014 Nov;31(11):611-9. doi: 10.1097/EJA.0000000000000122.
Axillary plexus blocks are usually guided by ultrasound, but alternative methods may be used when ultrasound equipment is lacking. For a nonultrasound-guided axillary block, the need for three injections has been questioned.
Could differences in block success between single, double and triple deposits methods be explained by differences in local anaesthetic distribution as observed by MRI?
A blinded and randomised controlled study.
Conducted at Oslo University Hospital, Rikshospitalet, Norway from 2009 to 2011.
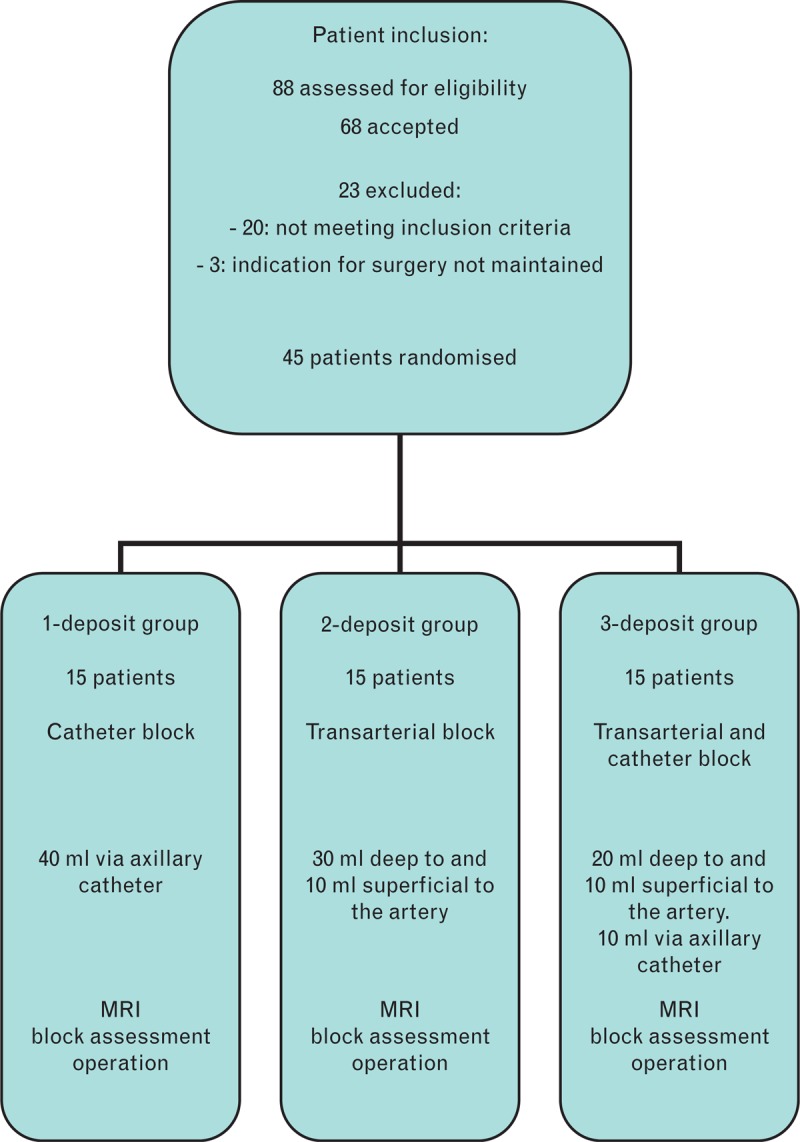
Forty-five ASA 1 to 2 patients scheduled for surgery were randomised to three equally sized groups. All patients completed the study.
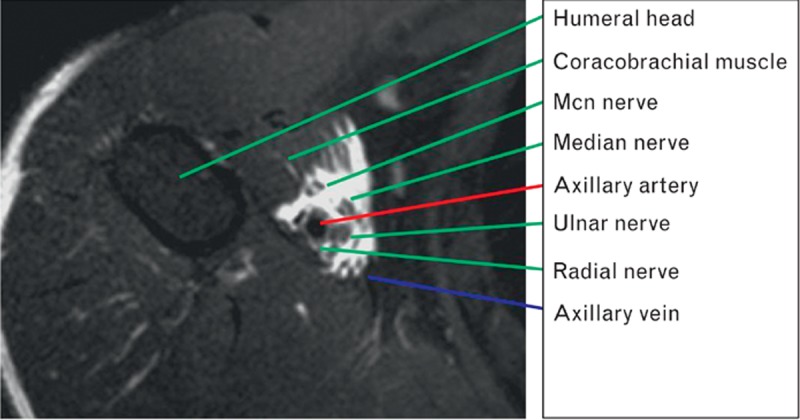
Patients in the single-deposit group had an injection through a catheter parallel to the median nerve. In the double-deposit group the patients received a transarterial block. In the triple-deposit group the injections of the two other groups were combined. Upon completion of local anaesthetic injection the patients were scanned by MRI, before clinical block assessment. The distribution of local anaesthetic was scored by its closeness to terminal nerves and cords of the brachial plexus, as seen by MRI. The clinical effect was scored by the degree of sensory block in terminal nerve innervation areas.
Sensory block effect and MRI distribution pattern.
The triple-deposit method had a higher success rate (100%) than the single-deposit method (67%) and the double-deposit method (67%) in blocking all cutaneous nerves distal to the elbow (P = 0.04). The patients in the triple-deposit group most often had the best MRI scores. For any nerve or cord, at least one of the single-deposit or double-deposit groups had a similarly high MRI score as the triple-deposit group.
Distal to the elbow, the triple-deposit method had the highest sensory block success rate. This could be explained to some extent by analysis of the magnetic resonance images.
ClinicalTrials.gov identifier: NCT01033006.
腋路臂丛神经阻滞通常在超声引导下进行,但在缺乏超声设备时可采用其他方法。对于非超声引导的腋路阻滞,是否需要三次注射一直存在疑问。
单次、两次和三次注射法之间的阻滞成功率差异能否通过MRI观察到的局麻药分布差异来解释?
一项双盲随机对照研究。
2009年至2011年在挪威奥斯陆大学医院Rikshospitalet进行。
45例拟行手术的ASA 1至2级患者被随机分为三个等规模组。所有患者均完成研究。
单次注射组患者通过与正中神经平行的导管进行注射。两次注射组患者接受经动脉阻滞。三次注射组则将其他两组的注射方法结合。在完成局麻药注射后,在进行临床阻滞评估前,患者接受MRI扫描。通过MRI观察,根据局麻药与臂丛神经终末神经和神经束的接近程度对局麻药分布进行评分。临床效果根据终末神经支配区域的感觉阻滞程度进行评分。
感觉阻滞效果和MRI分布模式。
在阻滞肘部远端所有皮神经方面,三次注射法的成功率(100%)高于单次注射法(67%)和两次注射法(67%)(P = 0.04)。三次注射组患者的MRI评分通常最高。对于任何神经或神经束,单次注射组或两次注射组中至少有一组的MRI评分与三次注射组相似。
在肘部远端,三次注射法的感觉阻滞成功率最高。这在一定程度上可以通过对磁共振图像的分析来解释。
ClinicalTrials.gov标识符:NCT01033006。