Rojas Blanca, Gallego Beatriz I, Ramírez Ana I, Salazar Juan J, de Hoz Rosa, Valiente-Soriano Francisco J, Avilés-Trigueros Marcelino, Villegas-Perez Maria P, Vidal-Sanz Manuel, Triviño Alberto, Ramírez José M
Instituto de Investigaciones Oftalmológicas Ramón Castroviejo, Facultad de Medicina, Pab VI, 4a, Avenida Complutense s/n, Universidad Complutense de Madrid, 28040 Madrid, Spain.
J Neuroinflammation. 2014 Jul 26;11:133. doi: 10.1186/1742-2094-11-133.
Glaucomatous optic neuropathy, a leading cause of blindness, can progress despite control of intraocular pressure - currently the main risk factor and target for treatment. Glaucoma progression shares mechanisms with neurodegenerative disease, including microglia activation. In the present model of ocular hypertension (OHT), we have recently described morphological signs of retinal microglia activation and MHC-II upregulation in both the untreated contralateral eyes and OHT eyes. By using immunostaining, we sought to analyze and quantify additional signs of microglia activation and differences depending on the retinal layer.
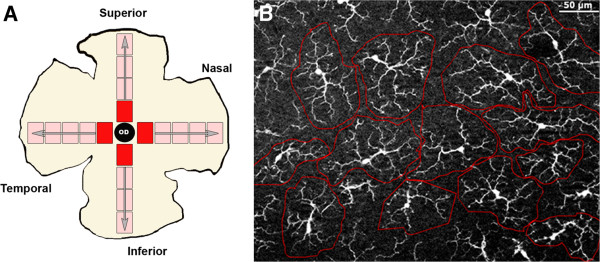
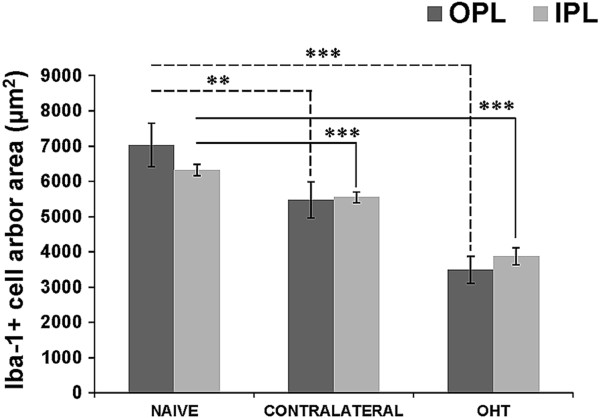
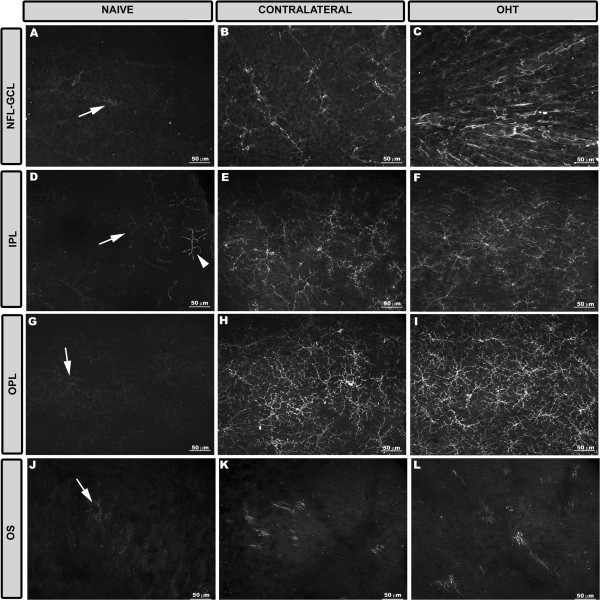
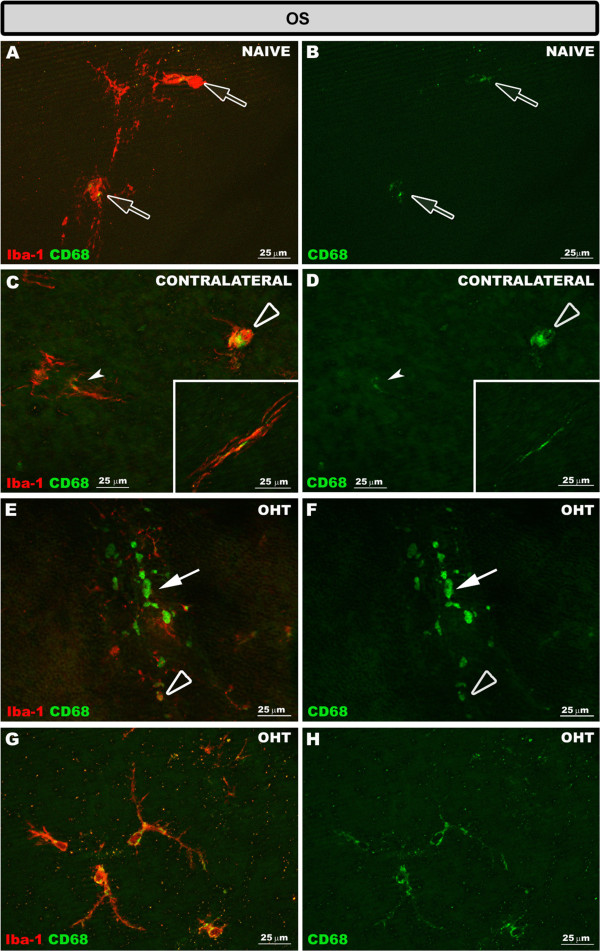
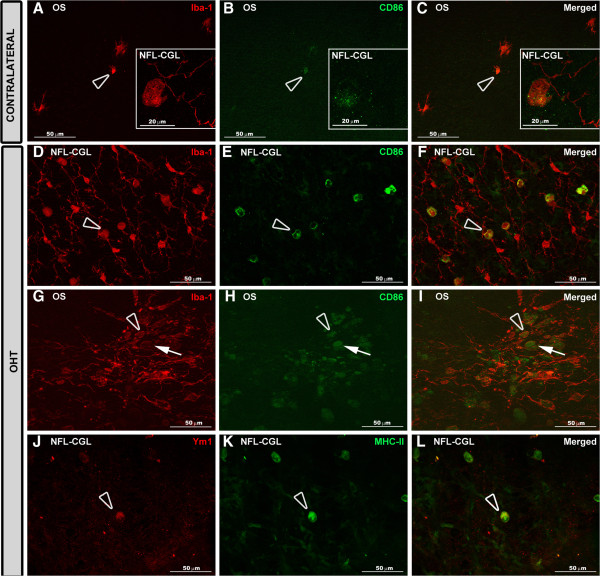
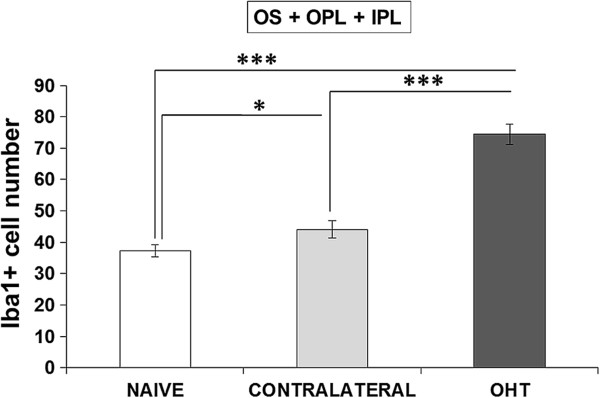
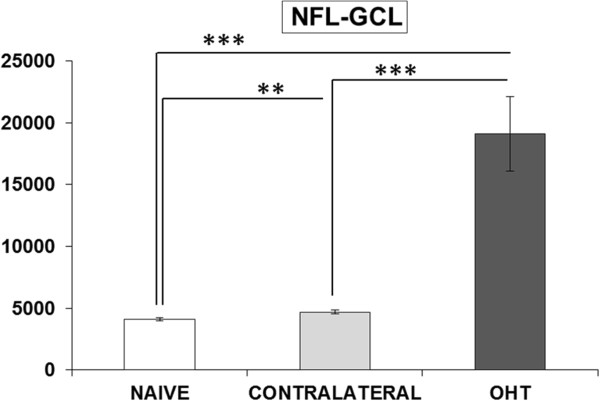
Two groups of adult Swiss mice were used: age-matched control (naïve, n = 12), and lasered (n = 12). In the lasered animals, both OHT eyes and contralateral eyes were analyzed. Retinal whole-mounts were immunostained with antibodies against Iba-1, MHC-II, CD68, CD86, and Ym1. The Iba-1+ cell number in the plexiform layers (PL) and the photoreceptor outer segment (OS), Iba-1+ arbor area in the PL, and area of the retina occupied by Iba-1+ cells in the nerve fiber layer-ganglion cell layer (NFL-GCL) were quantified.
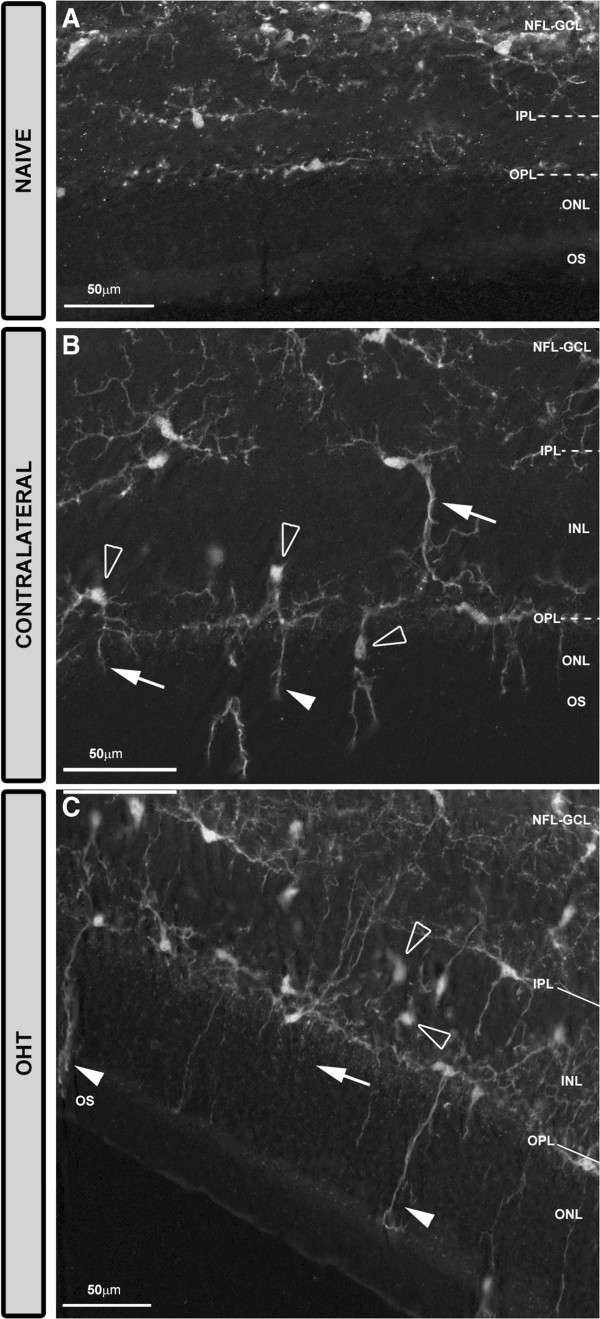
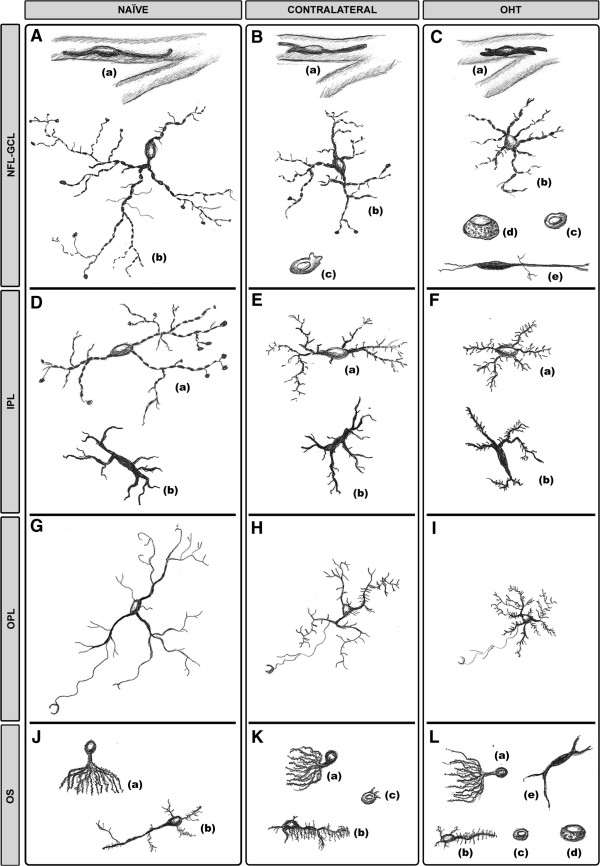
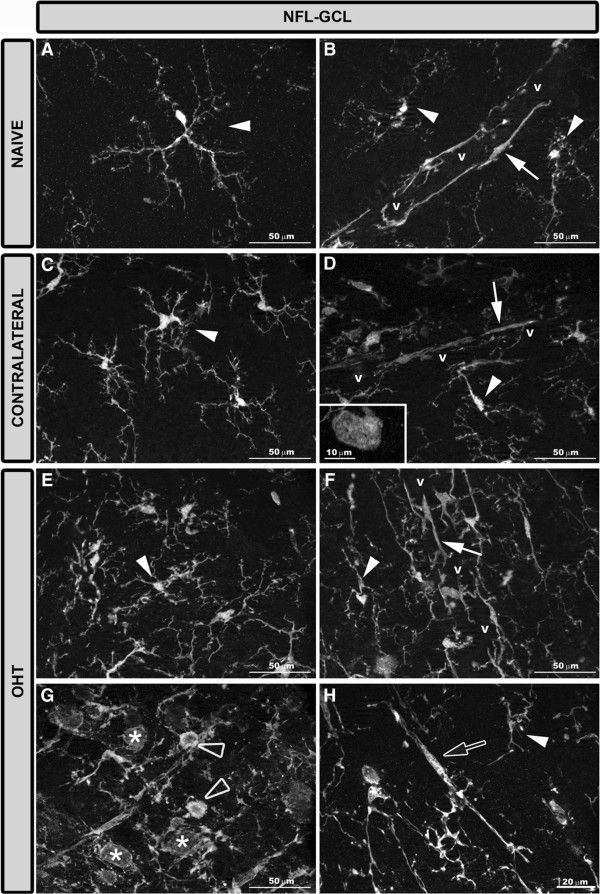
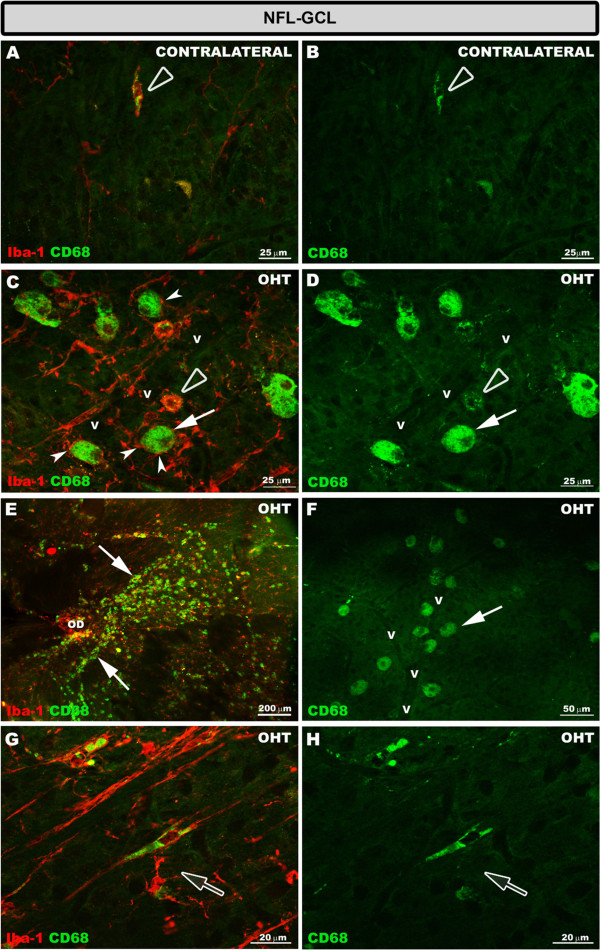
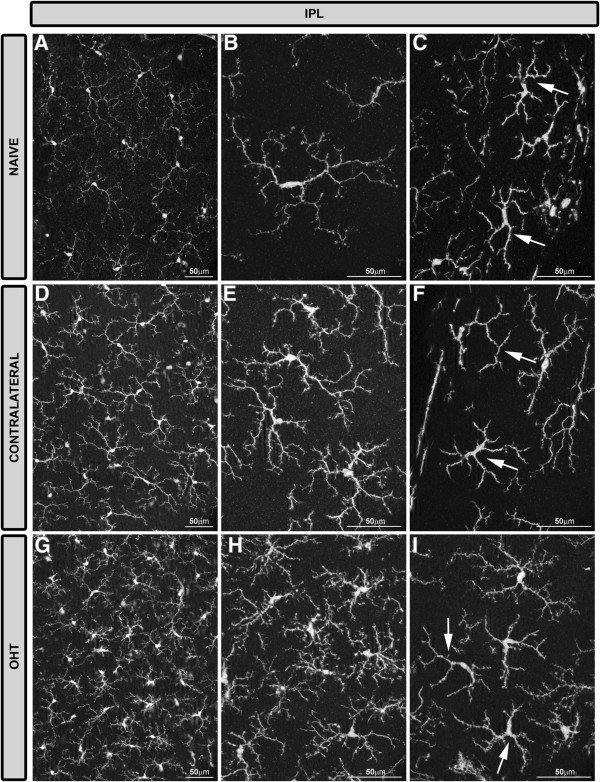
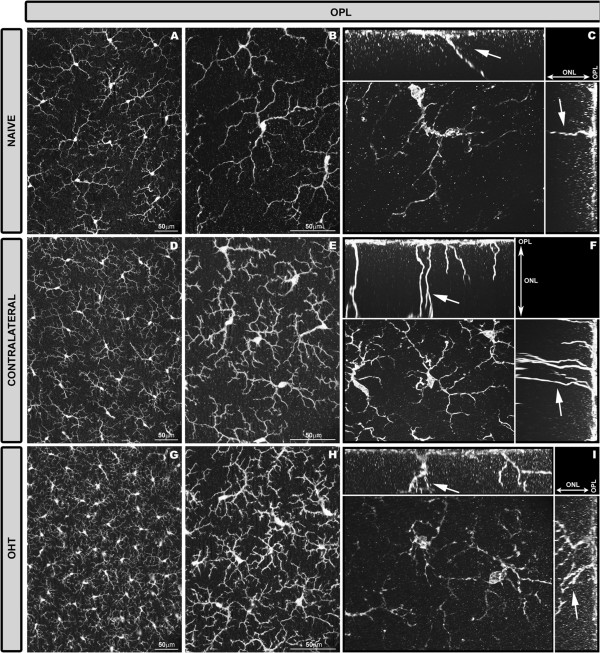
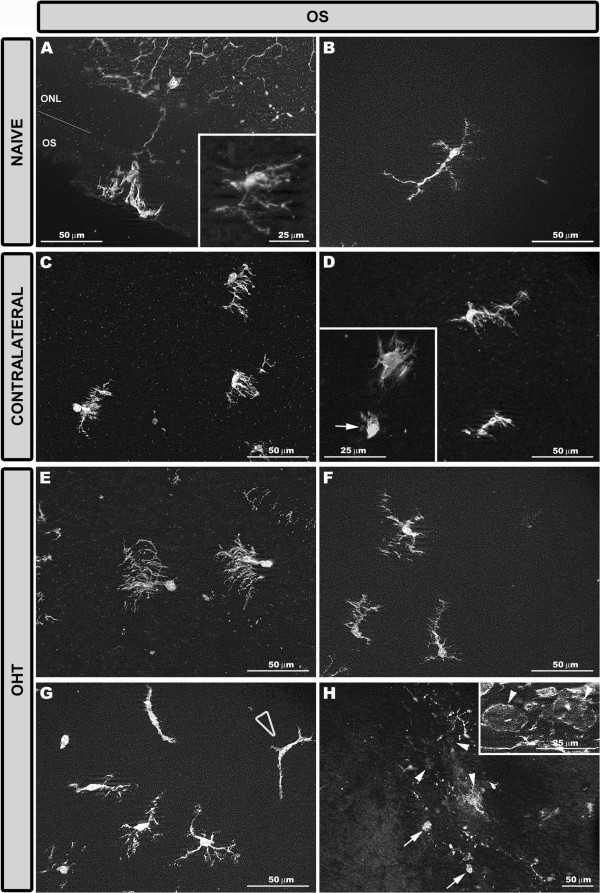
The main findings in contralateral eyes and OHT eyes were: i) ameboid microglia in the NFL-GCL and OS; ii) the retraction of processes in all retinal layers; iii) a higher level of branching in PL and in the OS; iv) soma displacement to the nearest cell layers in the PL and OS; v) the reorientation of processes in the OS; vi) MHC-II upregulation in all retinal layers; vii) increased CD68 immunostaining; and viii) CD86 immunolabeling in ameboid cells. In comparison with the control group, a significant increase in the microglial number in the PL, OS, and in the area occupied by Iba-1+ cells in the NFL-GCL, and significant reduction of the arbor area in the PL. In addition, rounded Iba-1+ CD86+ cells in the NFL-GCL, OS and Ym1+ cells, and rod-like microglia in the NFL-GCL were restricted to OHT eyes.
Several quantitative and qualitative signs of microglia activation are detected both in the contralateral and OHT eyes. Such activation extended beyond the GCL, involving all retinal layers. Differences between the two eyes could help to elucidate glaucoma pathophysiology.
青光眼性视神经病变是失明的主要原因之一,尽管眼压得到控制(目前眼压是主要危险因素和治疗靶点),病情仍可能进展。青光眼进展与神经退行性疾病有共同机制,包括小胶质细胞激活。在当前的高眼压(OHT)模型中,我们最近描述了未治疗的对侧眼和高眼压眼中视网膜小胶质细胞激活的形态学迹象以及MHC-II上调。通过免疫染色,我们试图分析和量化小胶质细胞激活的其他迹象以及视网膜各层之间的差异。
使用两组成年瑞士小鼠:年龄匹配的对照组(未处理,n = 12)和激光照射组(n = 12)。在激光照射的动物中,对高眼压眼和对侧眼均进行分析。视网膜全层标本用抗Iba-1、MHC-II、CD68、CD86和Ym1的抗体进行免疫染色。对视神经纤维层-神经节细胞层(NFL-GCL)中丛状层(PL)和光感受器外段(OS)的Iba-1+细胞数量、PL中Iba-1+树突面积以及Iba-1+细胞占据的视网膜面积进行量化。
对侧眼和高眼压眼的主要发现如下:i)NFL-GCL和OS中有阿米巴样小胶质细胞;ii)所有视网膜层的突起回缩;iii)PL和OS中分支水平更高;iv)PL和OS中细胞体向最近的细胞层移位;v)OS中突起重新定向;vi)所有视网膜层中MHC-II上调;vii)CD68免疫染色增加;viii)阿米巴样细胞中有CD86免疫标记。与对照组相比,PL、OS以及NFL-GCL中Iba-1+细胞占据区域的小胶质细胞数量显著增加,PL中树突面积显著减少。此外,NFL-GCL、OS中的圆形Iba-1+ CD86+细胞和Ym1+细胞以及NFL-GCL中的杆状小胶质细胞仅限于高眼压眼。
在对侧眼和高眼压眼中均检测到小胶质细胞激活的若干定量和定性迹象。这种激活超出了神经节细胞层,涉及所有视网膜层。两只眼睛之间的差异可能有助于阐明青光眼的病理生理学。