Kim Yoon Ji, Kim Yang Woo, Cheon Young Woo
Department of Plastic and Reconstructive Surgery, Gachon University Gil Medical Center, Gachon University School of Medicine, Incheon, Korea.
Arch Plast Surg. 2014 Jul;41(4):407-13. doi: 10.5999/aps.2014.41.4.407. Epub 2014 Jul 15.
Implant malposition can produce unsatisfactory aesthetic results after breast augmentation. The goal of this article is to identify aspects of the preoperative surgical planning and intraoperative flap fixation that can prevent implant malposition.
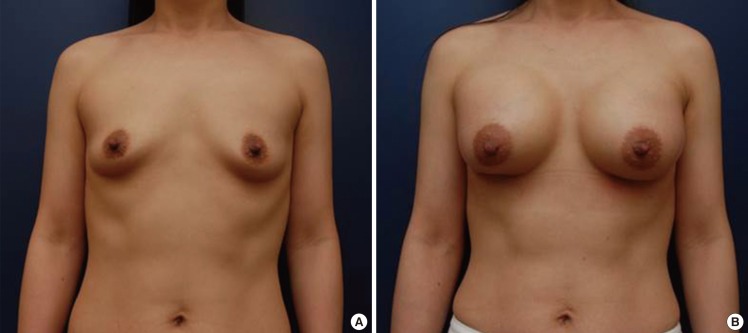
This study examined 36 patients who underwent primary dual plane breast augmentation through an inframammary incision between September 1, 2012 and January 31, 2013. Before the surgery, preoperative evaluation and design using the Randquist formula were performed. Each patient was evaluated retrospectively for nipple position relative to the breast implant and breast contour, using standardized preoperative and postoperative photographs. The average follow-up period was 10 months.
Seven of 72 breasts were identified as having implant malposition. These malpositions were divided into two groups. In relation to the new breast mound, six breasts had an inferiorly positioned and one breast had a superiorly positioned nipple-areolar complex. Two of these seven breasts were accompanied with an unsatisfactory breast contour.
We identified two main causes of implant malposition after inframammary augmentation mammaplasty. One cause was an incorrect preoperatively designed nipple to inframammary fold (N-IMF) distance. The breast skin and parenchyma quality, such as an extremely tight envelope, should be considered. If an extremely tight envelope is found, the preoperatively designed new N-IMF distance should be increased. The other main cause of malposition is failure of the fascial suture from Scarpa's fascia to the perichondrium through an inframammary incision. As well, when this fixation is performed, it should be performed directly downward to the perichondrium, rather than slanted in a cranial or caudal direction.
隆胸术后植入物位置不当会导致美学效果不佳。本文旨在确定术前手术规划和术中皮瓣固定中可预防植入物位置不当的方面。
本研究对2012年9月1日至2013年1月31日期间通过乳房下皱襞切口接受初次双平面隆胸手术的36例患者进行了检查。手术前,使用兰德奎斯特公式进行术前评估和设计。使用标准化的术前和术后照片,对每位患者乳头相对于乳房植入物和乳房轮廓的位置进行回顾性评估。平均随访期为10个月。
72个乳房中有7个被确定存在植入物位置不当。这些位置不当分为两组。相对于新的乳房隆起,6个乳房的乳头乳晕复合体位置较低,1个乳房的乳头乳晕复合体位置较高。这7个乳房中有2个伴有不满意的乳房轮廓。
我们确定了乳房下皱襞隆胸术后植入物位置不当的两个主要原因。一个原因是术前设计的乳头至乳房下皱襞(N-IMF)距离不正确。应考虑乳房皮肤和实质质量,如包膜极紧的情况。如果发现包膜极紧,术前设计的新N-IMF距离应增加。另一个主要的位置不当原因是通过乳房下皱襞切口从斯卡帕筋膜到软骨膜的筋膜缝合失败。同样,进行这种固定时,应直接向下固定至软骨膜,而不是向头侧或尾侧倾斜。