Department of Disease Control and Environmental Health, Makerere University School of Public Health, Kampala, Uganda.
Department of Medicine, Makerere University School of Medicine, Kampala, Uganda.
Lancet Glob Health. 2013 Sep;1(3):e137-45. doi: 10.1016/S2214-109X(13)70067-6. Epub 2013 Aug 23.
HIV counselling and testing and linkage to care are crucial for successful HIV prevention and treatment. Abbreviated counselling could save time; however, its effect on HIV risk is uncertain and methods to improve linkage to care have not been studied.
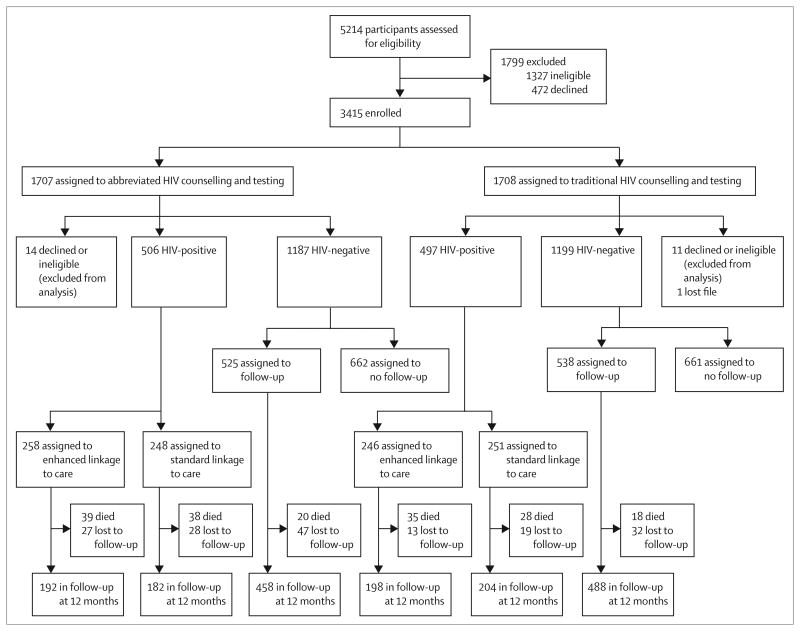
We did this factorial randomised controlled study at Mulago Hospital, Uganda. Participants were randomly assigned to abbreviated or traditional HIV counselling and testing; HIV-infected patients were randomly assigned to enhanced linkage to care or standard linkage to care. All study personnel except counsellors and the data officer were masked to study group assignment. Participants had structured interviews, given once every 3 months. We compared sexual risk behaviour by counselling strategy with a 6·5% non-inferiority margin. We used Cox proportional hazards analyses to compare HIV outcomes by linkage to care over 1 year and tested for interaction by sex. This trial is registered with ClinicalTrials.gov (NCT00648232).
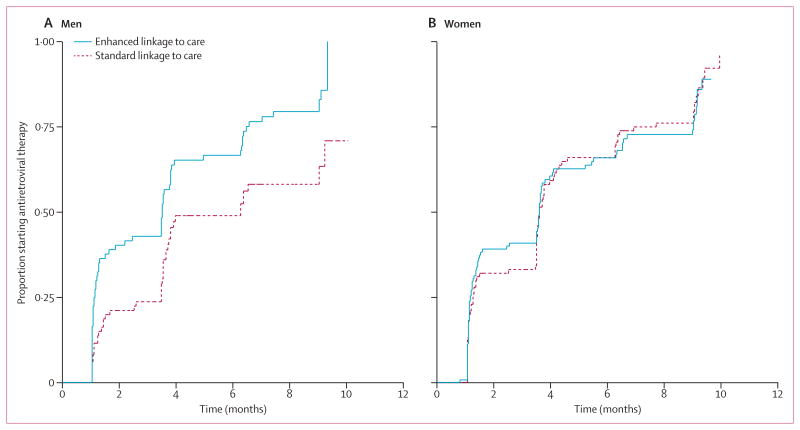
We enrolled 3415 participants; 1707 assigned to abbreviated counselling versus 1708 assigned to traditional. Unprotected sex with an HIV discordant or status unknown partner was similar in each group (232/823 [27·9%] vs 251/890 [28·2%], difference -0·3%, one-sided 95% CI 3·2). Loss to follow-up was lower for traditional counselling than for abbreviated counselling (adjusted hazard ratio [HR] 0·61, 95% CI 0·44-0·83). 1003 HIV-positive participants were assigned to enhanced linkage (n=504) or standard linkage to care (n=499). Linkage to care did not have a significant effect on mortality or receipt of co-trimoxazole. Time to treatment in men with CD4 cell counts of 250 cells per μL or fewer was lower for enhanced linkage versus standard linkage (adjusted HR 0·60, 95% CI 0·41-0·87) and time to HIV care was decreased among women (0·80, 0·66-0·96).
Abbreviated HIV counselling and testing did not adversely affect risk behaviour. Linkage to care interventions might decrease time to enrolment in HIV care and antiretroviral treatment and thus might affect secondary HIV transmission and improve treatment outcomes.
US National Institute of Mental Health.
艾滋病毒咨询和检测以及与护理的衔接对于成功预防和治疗艾滋病毒至关重要。简化咨询可以节省时间;然而,其对艾滋病毒风险的影响尚不确定,并且尚未研究改善与护理衔接的方法。
我们在乌干达的穆拉戈医院进行了这项两因素随机对照研究。参与者被随机分配接受简化或传统的艾滋病毒咨询和检测;艾滋病毒感染者被随机分配接受强化护理衔接或标准护理衔接。除咨询员外,所有研究人员和数据管理员都对研究组分配情况进行了掩盖。参与者每隔 3 个月进行一次结构化访谈。我们通过设定 6.5%的非劣效性边界,比较了不同咨询策略下的性行为风险。我们使用 Cox 比例风险分析比较了 1 年内通过护理衔接获得的艾滋病毒结果,并按性别检验了交互作用。该试验在 ClinicalTrials.gov(NCT00648232)注册。
我们共纳入 3415 名参与者;其中 1707 名分配到简化咨询组,1708 名分配到传统咨询组。与 HIV 不一致或未知状况的伴侣发生无保护性行为的情况在两组中相似(232/823[27.9%]与 251/890[28.2%],差异 0.3%,单侧 95%CI 3.2)。传统咨询组的失访率低于简化咨询组(校正后的风险比[HR]0.61,95%CI 0.44-0.83)。1003 名艾滋病毒阳性参与者被分配到强化衔接(n=504)或标准衔接护理(n=499)。衔接护理对死亡率或接受复方新诺明的影响没有显著差异。CD4 细胞计数为 250 个细胞/μL 或更低的男性中,强化衔接组的治疗时间比标准衔接组短(校正 HR 0.60,95%CI 0.41-0.87),女性的艾滋病毒护理时间也有所缩短(0.80,0.66-0.96)。
简化的艾滋病毒咨询和检测并未对行为风险产生不利影响。衔接护理干预措施可能会缩短艾滋病毒护理和抗逆转录病毒治疗的入组时间,从而可能影响二次艾滋病毒传播并改善治疗结果。
美国国家心理健康研究所。