Kent Shia T, Shimbo Daichi, Huang Lei, Diaz Keith M, Kilgore Meredith L, Oparil Suzanne, Muntner Paul
Department of Epidemiology, University of Alabama at Birmingham, Birmingham, Alabama, United States of America.
Center for Behavioral Cardiovascular Health, Department of Medicine, Columbia University Medical Center, New York, New York, United States of America.
PLoS One. 2014 Aug 25;9(8):e105888. doi: 10.1371/journal.pone.0105888. eCollection 2014.
After the 2003 publication of the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) guidelines, there was a 5-10% increase in patients initiating antihypertensive medication with a thiazide-type diuretic, but most patients still did not initiate treatment with this class. There are few contemporary published data on antihypertensive medication classes filled by patients initiating treatment.
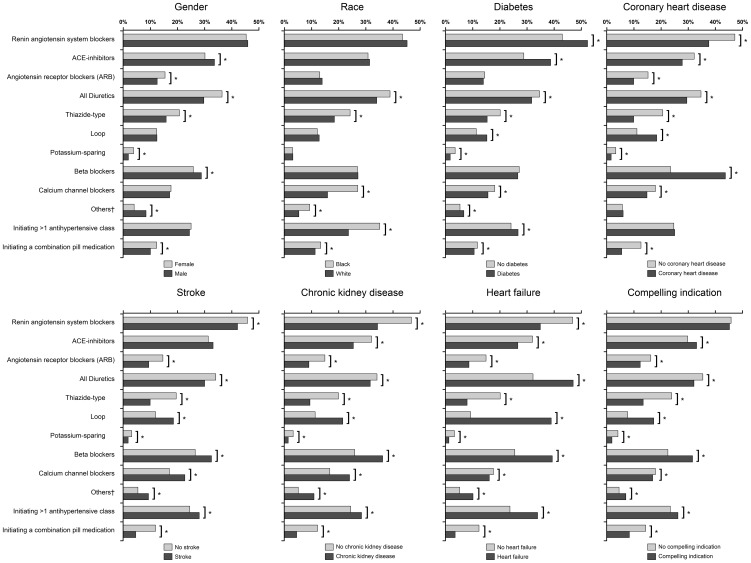
We used the 5% random Medicare sample to study the initiation of antihypertensive medication between 2007 and 2010. Initiation was defined by the first antihypertensive medication fill preceded by 365 days with no antihypertensive medication fills. We restricted our analysis to beneficiaries ≥ 65 years who had two or more outpatient visits with a hypertension diagnosis and full Medicare fee-for-service coverage for the 365 days prior to initiation of antihypertensive medication. Between 2007 and 2010, 32,142 beneficiaries in the 5% Medicare sample initiated antihypertensive medication. Initiation with a thiazide-type diuretic decreased from 19.2% in 2007 to 17.9% in 2010. No other changes in medication classes initiated occurred over this period. Among those initiating antihypertensive medication in 2010, 31.3% filled angiotensin-converting enzyme inhibitors (ACE-Is), 26.9% filled beta blockers, 17.2% filled calcium channel blockers, and 14.4% filled angiotensin receptor blockers (ARBs). Initiation with >1 antihypertensive medication class decreased from 25.6% in 2007 to 24.1% in 2010. Patients initiated >1 antihypertensive medication class most commonly with a thiazide-type diuretic and either an ACE-I or ARB.
These results suggest that JNC 7 had a limited long-term impact on the choice of antihypertensive medication class and provide baseline data prior to the publication of the 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8).
2003年美国国家联合委员会关于高血压预防、检测、评估及治疗的第七次报告(JNC 7)指南发布后,起始使用噻嗪类利尿剂进行抗高血压治疗的患者增加了5% - 10%,但大多数患者仍未开始使用此类药物治疗。关于开始治疗的患者所使用的抗高血压药物种类,目前当代公开的数据较少。
我们使用5%的医疗保险随机样本研究了2007年至2010年期间抗高血压药物的起始使用情况。起始使用定义为在首次开具抗高血压药物之前的365天内未开具过抗高血压药物。我们将分析限制在年龄≥65岁、有两次或更多次高血压诊断门诊就诊且在开始抗高血压药物治疗前365天有全额医疗保险按服务项目付费覆盖的受益人群。在2007年至2010年期间,5%医疗保险样本中的32142名受益人开始使用抗高血压药物。起始使用噻嗪类利尿剂的比例从2007年的19.2%降至2010年的17.9%。在此期间,起始使用的其他药物种类没有变化。在2010年开始使用抗高血压药物的人群中,31.3%开具了血管紧张素转换酶抑制剂(ACE - I),26.9%开具了β受体阻滞剂,17.2%开具了钙通道阻滞剂,14.4%开具了血管紧张素受体阻滞剂(ARB)。起始使用>1种抗高血压药物种类的比例从2007年的25.6%降至2010年的24.1%。患者起始使用>1种抗高血压药物种类最常见的是与噻嗪类利尿剂以及ACE - I或ARB联合使用。
这些结果表明,JNC 7对高血压药物种类选择的长期影响有限,并为2014年由第八届美国国家联合委员会(JNC 8)指定的专家小组发布的《成人高血压管理循证指南》提供了基线数据。