Callander Natalie, Markovina Stephanie, Eickhoff Jens, Hutson Paul, Campbell Toby, Hematti Peiman, Go Ronald, Hegeman Robert, Longo Walter, Williams Eliot, Asimakopoulos Fotis, Miyamoto Shigeki
University of Wisconsin Carbone Cancer Center, 600 Highland Ave, Madison, WI, 53792, USA,
Cancer Chemother Pharmacol. 2014 Oct;74(4):875-82. doi: 10.1007/s00280-014-2550-5. Epub 2014 Aug 29.
Retreatment with bortezomib (B) is often considered for patients with relapsed multiple myeloma (MM), but this strategy is hindered by uncertainty of response and emergence of B-induced peripheral neuropathy (PN). We incorporated acetyl-L-carnitine (ALCAR) to prevent PN and allow for adequate dosing. We also investigated the correlation between B-inducible NF-κB activation and response to therapy.
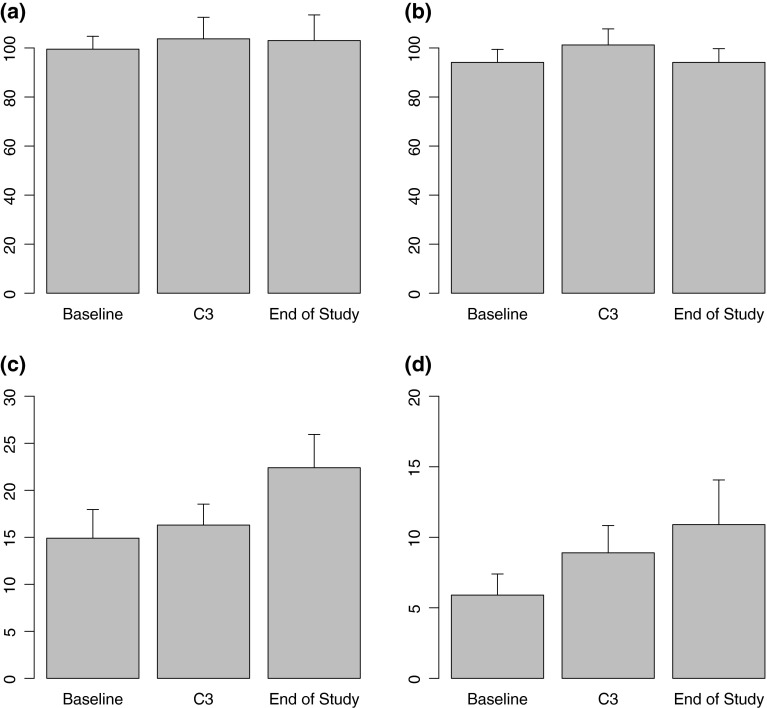
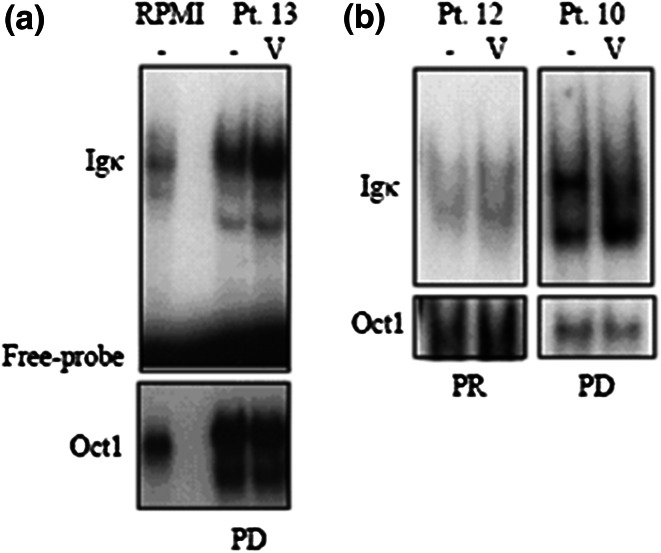
Nineteen patients with relapsed/refractory MM received up to 8 cycles of intravenous bortezomib, doxorubicin and oral low-dose dexamethasone (BDD) to evaluate response and toxicity. Thirteen additional patients received prophylactic ALCAR (BDD-A). Patients receiving BDD-A were evaluated by FACT-GOG-TX, FACIT-Fatigue, Neuropathic Pain index (NPI) and Grooved Pegboard (GP) testing. Primary MM cells from 11 patients were tested for B-inducible NF-κB activation.
Seventy-six percent of subjects were refractory to previous treatment, 39% refractory to bortezomib. Median cycles received were 5. CR + PR for the entire group were 53% and did not differ between groups. Incidence of ≥3 PN was 32% in the BDD group versus 15 % in the BDD-A group (p = ns). Patient-reported fatigue and PN measured by FACT-GOG-TX increased throughout the treatment period in the BDD-A group, although time to complete GP testing declined. In a sub-study examining constitutive bortezomib-inducible NF-κB activity in primary subject-specific MM cells, the presence of NF-κB activation correlated with lower likelihood of response.
Addition of ALCAR to BDD did not alter the incidence or severity of PN in relapsed MM patients receiving a B-based regimen. Bortezomib-inducible NF-κB activation in patient-derived primary MM cells may be associated with poorer response.
复发的多发性骨髓瘤(MM)患者常考虑使用硼替佐米(B)进行再治疗,但该策略因反应的不确定性和硼替佐米诱导的周围神经病变(PN)的出现而受到阻碍。我们加入乙酰左旋肉碱(ALCAR)以预防PN并实现足够的剂量。我们还研究了硼替佐米诱导的NF-κB激活与治疗反应之间的相关性。
19例复发/难治性MM患者接受了多达8个周期的静脉注射硼替佐米、阿霉素和口服低剂量地塞米松(BDD),以评估反应和毒性。另外13例患者接受了预防性ALCAR(BDD-A)。接受BDD-A的患者通过FACT-GOG-TX、FACIT-疲劳、神经性疼痛指数(NPI)和带槽钉板(GP)测试进行评估。对11例患者的原发性MM细胞进行硼替佐米诱导的NF-κB激活测试。
76%的受试者对先前治疗耐药,39%对硼替佐米耐药。接受的中位周期数为5个。整个组的完全缓解(CR)+部分缓解(PR)率为53%,两组之间无差异。BDD组≥3级PN的发生率为32%,而BDD-A组为15%(p=无显著性差异)。在BDD-A组中,通过FACT-GOG-TX测量的患者报告的疲劳和PN在整个治疗期间增加,尽管完成GP测试的时间缩短。在一项检查原发性受试者特异性MM细胞中组成性硼替佐米诱导的NF-κB活性的亚研究中,NF-κB激活的存在与较低的反应可能性相关。
在接受基于硼替佐米方案的复发MM患者中,在BDD中加入ALCAR不会改变PN的发生率或严重程度。患者来源的原发性MM细胞中硼替佐米诱导NF-κB激活可能与较差的反应相关。