Penzkofer Tobias, Donandt Eva, Isfort Peter, Allmendinger Thomas, Kuhl Christiane K, Mahnken Andreas H, Bruners Philipp
Department of Diagnostic and Interventional Radiology, Aachen University Hospital, RWTH Aachen University, Pauwelsstr, 30, 52074 Aachen, Germany.
BMC Med Imaging. 2014 Sep 1;14:30. doi: 10.1186/1471-2342-14-30.
To investigate the impact of high pitch cardiac CT vs. retrospective ECG gated CT on the quantification of calcified vessel stenoses, with assessment of the influence of tube voltage, reconstruction kernel and heart rate.
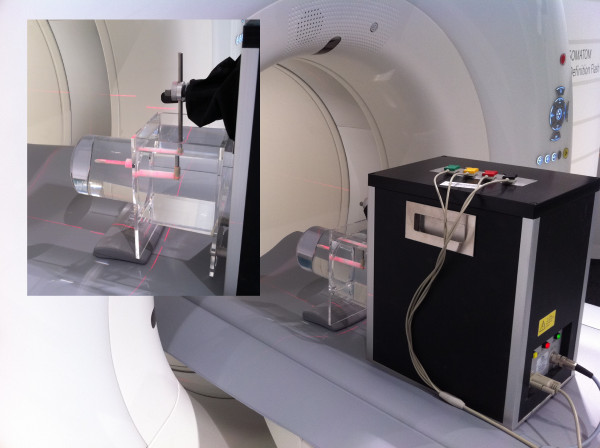
A 4D cardiac movement phantom equipped with three different plaque phantoms (12.5%, 25% and 50% stenosis at different calcification levels), was scanned with a 128-row dual source CT scanner, applying different trigger types (gated vs. prospectively triggered high pitch), tube voltages (100-120 kV) and heart rates (50-90 beats per minute, bpm). Images were reconstructed using different standard (B26f, B46f, B70f) and iterative (I26f, I70f) convolution kernels. Absolute and relative plaque sizes were measured and statistically compared. Radiation dose associated with the different methods (gated vs. high pitch, 100 kV vs. 120 kV) were compared.
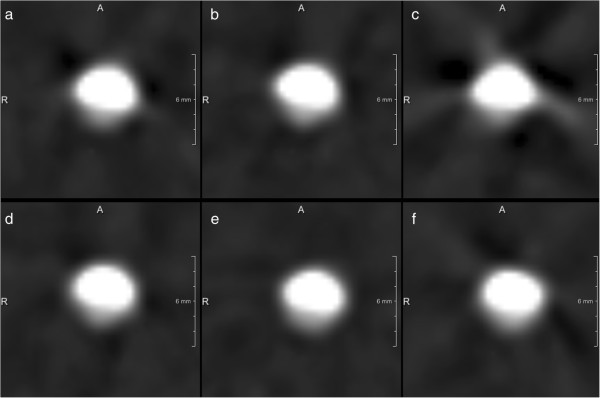
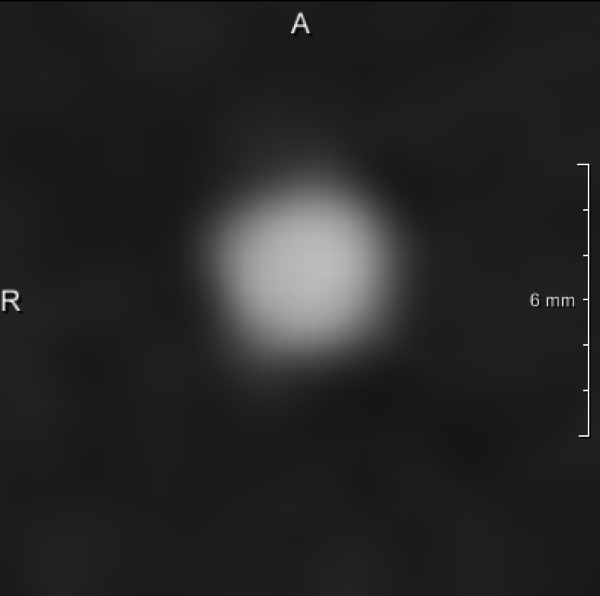
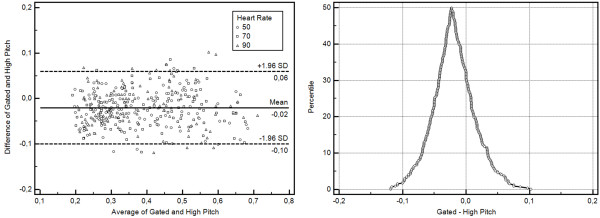
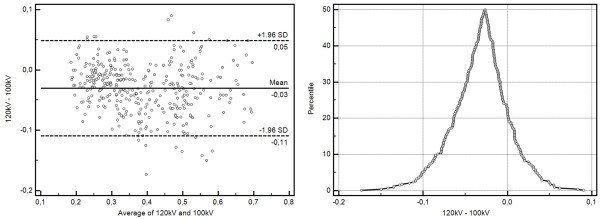
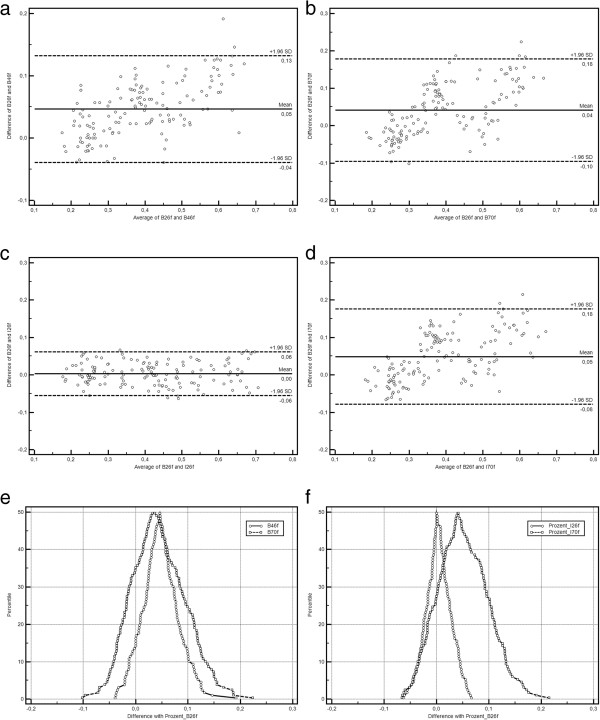
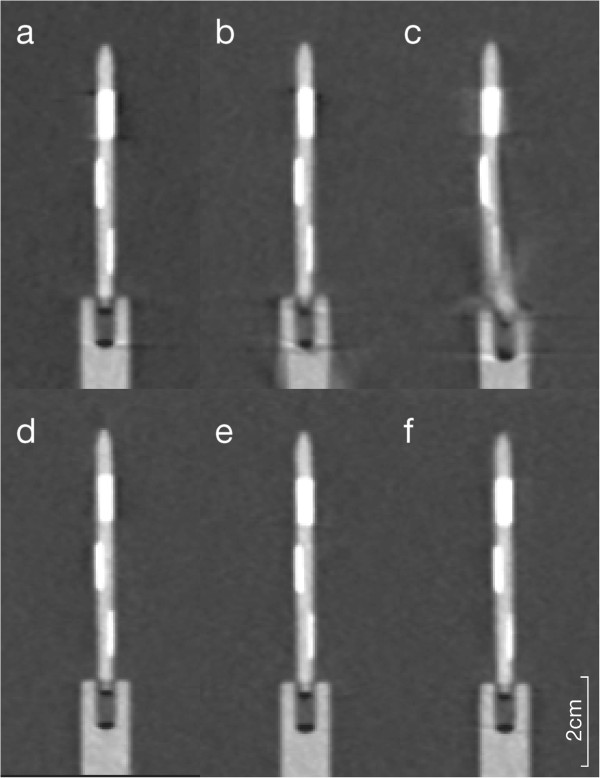
Compared to the known diameters of the phantom plaques and vessels both CT-examination techniques overestimated the degrees of stenoses. Using the high pitch CT-protocol plaques appeared larger (0.09 ± 0.31 mm, 2 ± 8 percent points, PP) in comparison to the ECG-gated CT-scans. Reducing tube voltage had a similar effect, resulting in higher grading of the same stenoses by 3 ± 8 PP. In turn, sharper convolution kernels lead to a lower grading of stenoses (differences of up to 5%). Pairwise comparison of B26f and I26f, B46f and B70f, and B70f and I70f showed differences of 0-1 ± 6-8 PP of the plaque depiction. Motion artifacts were present only at 90 bpm high pitch experiments. High-pitch protocols were associated with significantly lower radiation doses compared with the ECG-gated protocols (258.0 mGy vs. 2829.8 mGy CTDIvol, p ≤ 0.0001).
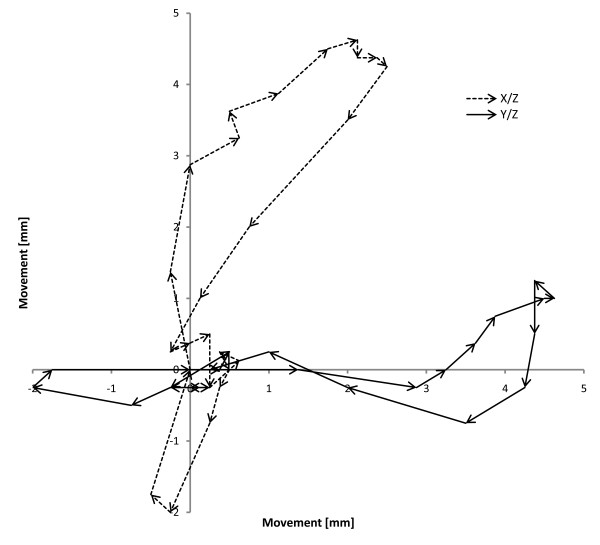
Prospectively triggered high-pitch cardiac CT led to an overestimation of plaque diameter and degree of stenoses in a coronary phantom. This overestimation is only slight and probably negligible in a clinical situation. Even at higher heart rates high pitch CT-scanning allowed reliable measurements of plaque and vessel diameters with only slight differences compared ECG-gated protocols, although motion artifacts were present at 90 bpm using the high pitch protocols.
研究高螺距心脏CT与回顾性心电图门控CT对钙化血管狭窄定量的影响,并评估管电压、重建核和心率的影响。
使用配备三种不同斑块模型(不同钙化水平下狭窄率分别为12.5%、25%和50%)的4D心脏运动模型,通过128排双源CT扫描仪进行扫描,应用不同的触发类型(门控与前瞻性触发高螺距)、管电压(100 - 120 kV)和心率(每分钟50 - 90次心跳,bpm)。使用不同的标准(B26f、B46f、B70f)和迭代(I26f、I70f)卷积核重建图像。测量并统计比较绝对和相对斑块大小。比较不同方法(门控与高螺距,100 kV与120 kV)相关的辐射剂量。
与模型斑块和血管的已知直径相比,两种CT检查技术均高估了狭窄程度。与心电图门控CT扫描相比,使用高螺距CT方案时斑块显得更大(0.09 ± 0.31 mm,2 ± 8个百分点,PP)。降低管电压有类似效果,导致相同狭窄的分级更高3 ± 8 PP。反过来,更锐利的卷积核导致狭窄分级更低(差异高达5%)。B26f与I26f、B46f与B70f以及B70f与I70f的两两比较显示斑块描绘差异为0 - 1 ± 6 - 8 PP。仅在90 bpm高螺距实验中出现运动伪影。与心电图门控方案相比,高螺距方案的辐射剂量显著更低(容积CT剂量指数CTDIvol为258.0 mGy对2829.8 mGy,p ≤ 0.0001)。
前瞻性触发的高螺距心脏CT导致冠状动脉模型中斑块直径和狭窄程度的高估。这种高估在临床情况下仅轻微且可能可忽略不计。即使在较高心率下,高螺距CT扫描也能可靠测量斑块和血管直径,与心电图门控方案相比差异仅轻微,尽管使用高螺距方案在90 bpm时存在运动伪影。