Cinotti Raphaël, Ichai Carole, Orban Jean-Christophe, Kalfon Pierre, Feuillet Fanny, Roquilly Antoine, Riou Bruno, Blanloeil Yvonnick, Asehnoune Karim, Rozec Bertrand
Crit Care. 2014 Sep 5;18(5):498. doi: 10.1186/s13054-014-0498-9.
Hyperglycemia is a marker of poor prognosis in severe brain injuries. There is currently little data regarding the effects of intensive insulin therapy (IIT) on neurological recovery.
A sub-group analysis of the randomized-controlled CGAO-REA study (NCT01002482) in surgical intensive care units (ICU) of two university hospitals. Patients with severe brain injury, with an expected ICU length of stay ≥ 48 hours were included. Patients were randomized between a conventional glucose management group (blood glucose target between 5.5 and 9 mmol.L(-1)) and an IIT group (blood glucose target between 4.4 and 6 mmol.L(-1)). The primary outcome was the day-90 neurological outcome evaluated with the Glasgow outcome scale.
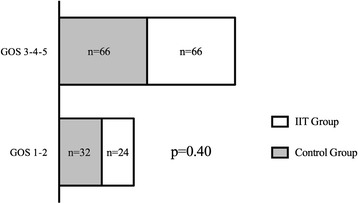
A total of 188 patients were included in this analysis. In total 98 (52%) patients were randomized in the control group and 90 (48%) in the IIT group. The mean Glasgow coma score at baseline was 7 (± 4). Patients in the IIT group received more insulin (130 (68 to 251) IU versus 74 (13 to 165) IU in the control group, P = 0.01), had a significantly lower morning blood glucose level (5.9 (5.1 to 6.7) mmol.L(-1) versus 6.5 (5.6 to 7.2) mmol.L(-1), P <0.001) in the first 5 days after ICU admission. The IIT group experienced more episodes of hypoglycemia (P < 0.0001). In the IIT group 24 (26.6%) patients had a favorable neurological outcome (good recovery or moderate disability) compared to 31 (31.6%) in the control group (P = 0.4). There were no differences in day-28 mortality. The occurrence of hypoglycemia did not influence the outcome.
In this sub-group analysis of a large multicenter randomized trial, IIT did not appear to alter the day-90 neurological outcome or ICU morbidity in severe brain injured patients or ICU morbidity.
高血糖是重度脑损伤预后不良的一个指标。目前关于强化胰岛素治疗(IIT)对神经功能恢复影响的数据很少。
对两家大学医院外科重症监护病房(ICU)进行的随机对照CGAO - REA研究(NCT01002482)进行亚组分析。纳入预期在ICU住院时间≥48小时的重度脑损伤患者。患者被随机分为传统血糖管理组(血糖目标值在5.5至9 mmol.L⁻¹之间)和IIT组(血糖目标值在4.4至6 mmol.L⁻¹之间)。主要结局是采用格拉斯哥预后量表评估的90天神经功能结局。
本分析共纳入188例患者。总共98例(52%)患者被随机分配至对照组,90例(48%)患者被随机分配至IIT组。基线时格拉斯哥昏迷评分平均为7分(±4)。IIT组患者接受了更多胰岛素治疗(130(68至251)IU,而对照组为74(13至165)IU,P = 0.01),在入住ICU后的前5天,其早晨血糖水平显著更低(5.9(5.1至6.7)mmol.L⁻¹,而对照组为6.5(5.6至7.2)mmol.L⁻¹,P <0.001)。IIT组发生低血糖的次数更多(P <0.0001)。IIT组有24例(26.6%)患者神经功能结局良好(恢复良好或中度残疾),而对照组为31例(31.6%)(P = 0.4)。28天死亡率无差异。低血糖的发生并未影响结局。
在这项大型多中心随机试验的亚组分析中,IIT似乎并未改变重度脑损伤患者的90天神经功能结局或ICU发病率。